
- Overview
- Prognosis
- Case Examples
- Differential diagnosis (active NAAION)
- Differential diagnosis (previous NAAION)
Overview
NAAION typically presents with a swollen disc with a flame-shaped haemorrhage in the acute phase. The extent of disc oedema is usually segmental rather than diffuse. A key feature that differentiates NAAION from AION is that the disc oedema is hyperaemic rather than pallid. Following the acute phase, disc pallor and RNFL loss can be seen in the region of previous oedema.
Sudden, painless unilateral vision loss is usually noted and may vary in severity with 4-14% of patients having severe loss and 31% - 73% having vision of 6/18 (20/60) or better. A relative afferent pupillary defect (RAPD) is present in the affected eye.
NAAION occurs in “at risk” discs – that is, discs that are crowded and have a small cup-to-disc ratio. The obstruction of the short posterior ciliary arteries cause ischaemia and axonal oedema. The swelling of the axons within a fixed space causes an already crowded disc to become more congested, compressing the capillaries and leading to additional ischaemia (compartment syndrome).
The blood supply to the optic disc is delivered by the ring of Zinn-Haller which is actually made up of 2 parts – one supplying the superior half of the disc and the other supplying the inferior half. Typically, only one of these is blocked, therefore the disc oedema is typically sectoral. Visual field loss is altitudinal in most cases.
NAAION is most commonly seen in patients over 50 years of age with underlying vascular disease(s) such as hypertension, diabetes or hypercholesterolemia. Sleep apnoea also has a strong association with NAAION (up to 80% of NAAION patients report having sleep apnoea).
Prognosis
NAAION usually stabilises over 2-3 months and visual acuity may improve by up to 3 lines. Recurrence is rare (5%) with the likely explanation being that the RNFL loss associated with NAAION reduces overcrowding at the optic nerve head.
However, the other eye may subsequently become involved in 59% of cases, although the time between eyes is highly variable.
While corticosteroids are used to treat AAION, there is currently no widely accepted treatment for NAAION.
Case Examples
-
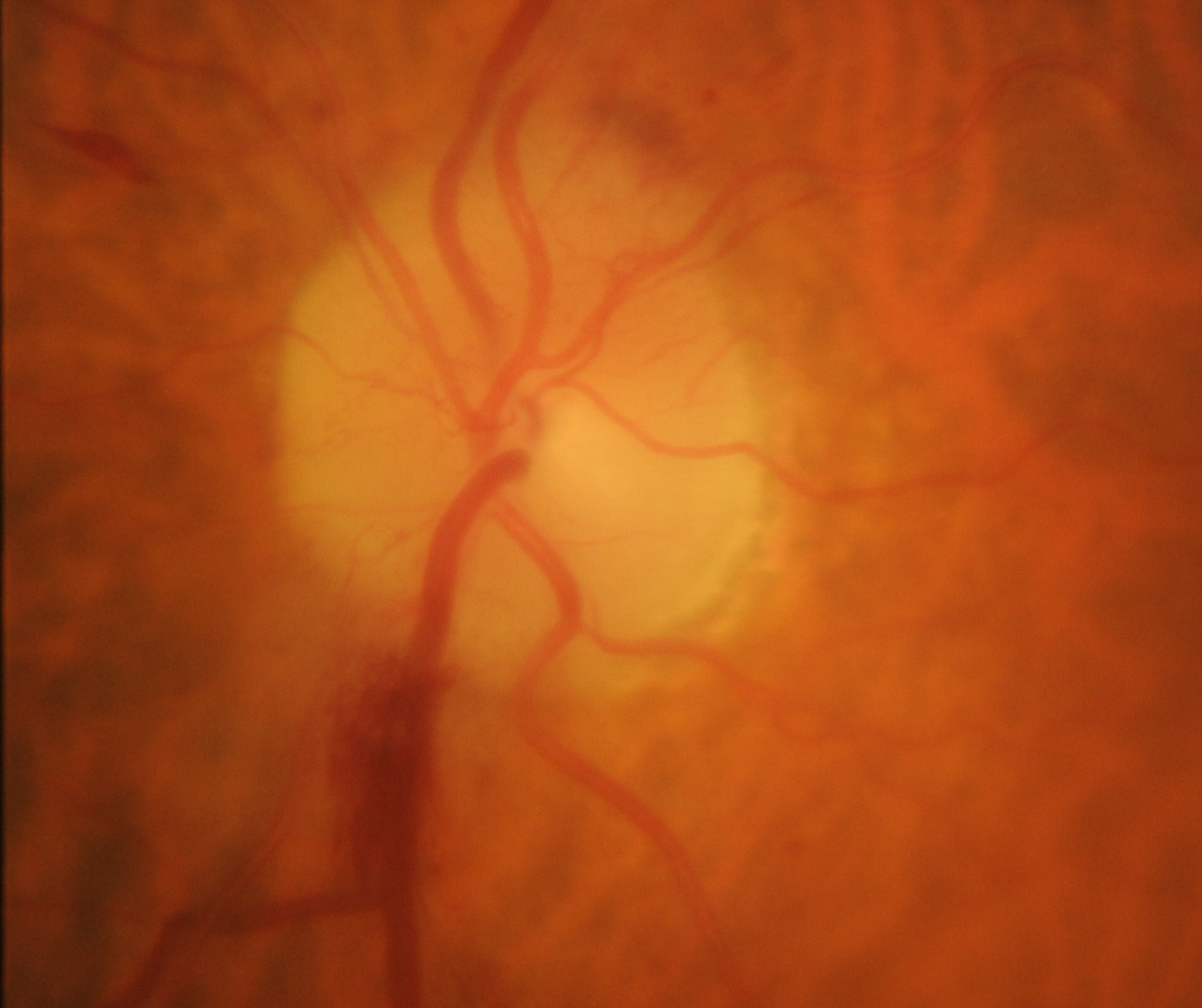
Case 1: Active NAAION
A 68 year old Middle Eastern male with type 2 diabetes, diagnosed 6 years previously. His HbA1c ranges from 5.7-6.1%. His best corrected visual acuity is 6/6 (20/20) in the right eye and 6/12 (20/40) in the left eye.
-
Case 2: Previous NAAION
A 65 year old Caucasian female with systemic hypertension, renal failure and type 2 diabetes (most recent HbA1c 5.6%). Best corrected visual acuity is 6/7.5-2 (20/25-2) in both eyes. She reports a period of vision loss in the right eye 9 years previous.
-
Case 3: Previous NAAION
A 76 year old Caucasian male who is being treated for systemic hypertension. He was diagnosed with a non-arteritic anterior ischaemic optic neuropathy 10 years prior. His best corrected visual acuity is 6/9.5 (20/32) in each eye.