
- Overview
- Acute Papilloedema
- Chronic Papilloedema
- Case Examples
- Differential Diagnosis
- Related topics
- References
Overview
Papilloedema presents as bilateral swelling of the optic nerve head (ONH) secondary to increased intracranial pressure (ICP). The swelling of the ONH may be asymmetric and can develop over a few hours to weeks. Papilloedema requires an accurate diagnosis and urgent management as it is potentially sight and life threatening.
Raised ICP causes a reduction in brain perfusion and results in ischaemic damage. The increased pressure is transferred down the optic nerve sheath from the intracranial cavity, causing axoplasmic flow stasis and ischaemia. This leads to axonal oedema and interstitial fluid accumulation within the ONH tissue, resulting in swelling and elevation.
ICP can be caused by several mechanisms including an increase in brain volume (e.g. due to trauma or ischaemia), an increase in mass (e.g. intracranial tumours), an increase in cerebrospinal fluid (e.g. due to increased production or decreased absorption), an increase in blood volume (e.g. cardiovascular complications), the use of some medications and skull deformities. It may also have no known cause, termed idiopathic intracranial hypertension (IIH). IIH predominately affects women of childbearing age who are overweight however it may affect others outside of this group including children, the elderly and those without obesity. It may also be associated with recent weight change.
Symptoms of papilloedema can vary from person to person, but may include the following: a headache worse in morning upon waking or being recumbent, transient visual loss, diplopia, pulsatile tinnitus, nausea or vomiting. Central vision acuity is relatively well preserved in most cases.
Malignant hypertension is another cause of papilloedema and that is covered elsewhere in this resource. Please use the link at the bottom of the page to navigate to this page.
Acute Papilloedema
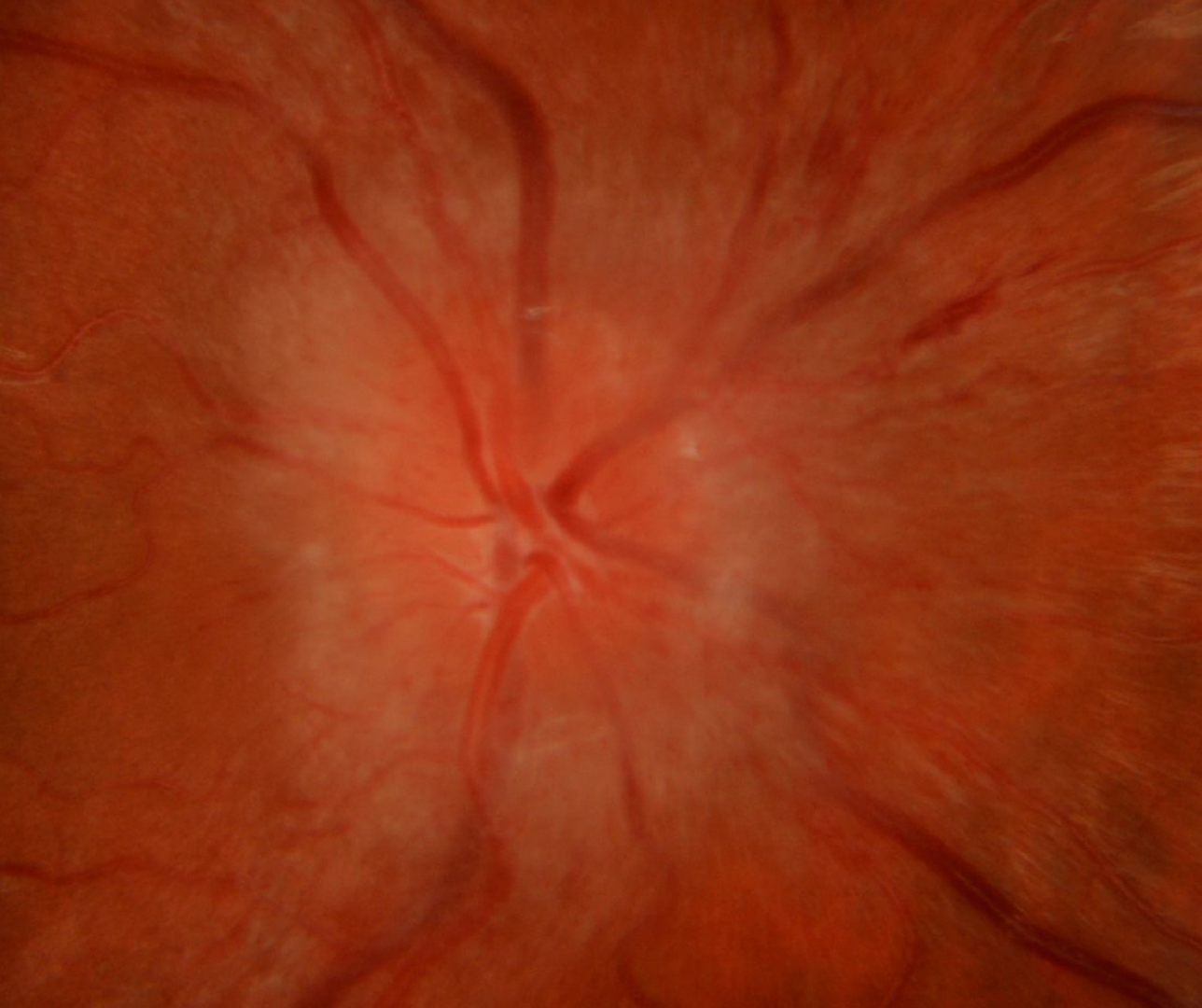
Acute papilloedema is characterised by blurry disc margins due to a thickened peripapillary RNFL and elevation of the optic disc on clinical examination. Additional clinical features include increased vessel tortuosity, dilated disc capillaries, vessel obscuration, peripapillary haemorrhages, loss of spontaneous venous pulsation, adjacent retinal and choroidal folds (Paton's folds) and disc hyperaemia.
Fundus autofluorescence imaging shows dense hypo-autofluorescence extending beyond the peripapillary area.
OCT imaging shows marked elevation of the ONH and thickening of the RNFL with "rainbow fringes" on the RNFL analysis. In some cases, a triangular shaped hypo-reflective “wedge” may be seen in the peripapillary region (termed a “V contour), however this is not always present. There may also be cystic spaces in the peripapillary retina and an anterior bowing of the RPE/ Bruch's membrane layer at the optic canal opening.
Visual field testing in the acute stages shows enlargement of the blind spot.
Chronic Papilloedema
In chronic cases, visual acuity can be affected and visual fields can constrict. Optociliary shunts may also be present.
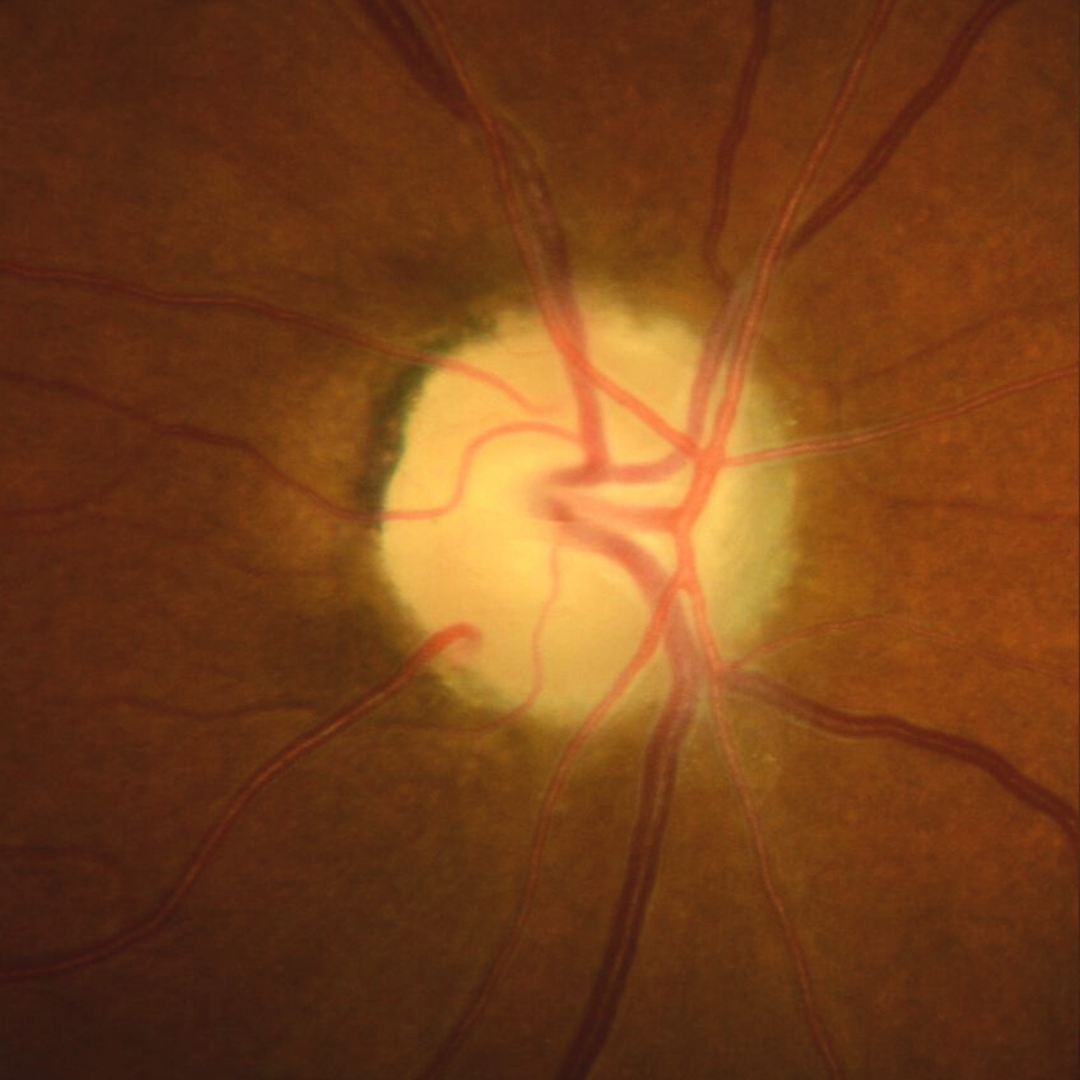
Continued pressure on the ONH results in the death of axons and subsequently secondary optic atrophy. Disc pallor with RNFL thinning will occur and can be associated with visual field defects. The field defects can be unpredictable however the papillomacular bundle is typically spared until the later stages of disease, so visual acuity usually remains relatively good until this time.
A link to more information on secondary optic atrophy is included at the bottom of this page.
Case Examples
-
Case 1: Obvious papilloedema and IIH
A 23 year old overweight Caucasian female with best corrected visual acuity of 6/7.5 (20/25) in both eyes. She has symptoms of headaches (worse in the morning), nausea and blurred vision.
-
Case 2: Subtle papilloedema and IIH
A 38 year old, obese female with worsening "sensations" in her peripheral vision, worse on waking in the morning. The patient has a complex medical history including type 2 diabetes, sleep apnoea and systemic hypertension. Her best corrected visual acuity was 6/6+ (20/20+) in both eyes. This patient was referred urgently to hospital and the diagnosis of IIH was confirmed.
Fundus photos (right and left eye)
More infoRed free images (right and left eye)
More infoStereoscopic image (right optic disc)
More infoStereoscopic image (left optic disc)
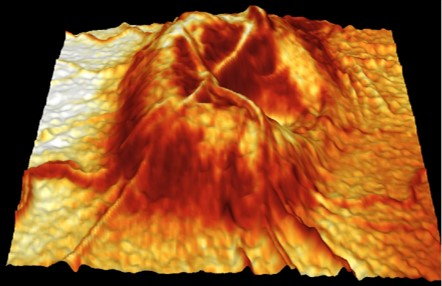
More info3-D representation of the optic nerves
More infoSpectralis OCT volume and line scans (right eye)
More infoSpectralis OCT volume and line scans (left eye)
More infoCirrus RNFL analysis
More infoCirrus Ganglion Cell Analysis
More info -
Case 3: Subtle papilloedema
A 24 year old Middle Eastern male with symptoms of headaches on wakening that last 1-2 hours and intermittent visual disturbances in his temporal vision. He reports no nausea or vomiting and his best corrected visual acuity is 6/6 (20/20) in each eye. This patient was referred urgently to hospital and a diagnosis of papilloedema was confirmed.
Fundus photos (right and left eye)
More infoRed free images (right and left eye)
More infoStereoscopic image (right optic disc )
More infoStereoscopic image (left optic disc)
More infoSpectralis OCT line scans (right optic disc)
More infoSpectralis OCT line scans (left optic disc)
More infoCirrus RNFL analysis
More info -
Case 4: Resolving papilloedema
A 46 year old Middle Eastern male with best corrected visual acuity of 6/6+ (20/20+) in each eye. He reports mild symptoms of nausea in recent days. The clinical findings were suspicious for papilloedema at his initial visit and he was promptly referred for further investigations. Subsequent testing revealed raised intracranial pressure and a lumbar puncture was undertaken. The following images capture the resolution of the clinical signs of papilloedema over a period of 7 years.
Fundus photos and fundus autofluorescence images (initial presentation)
More infoCirrus RNFL analysis
More infoFlicker presentation - retinal photos pre- and post-lumbar puncture
More infoFlicker presentation - resolution of papilloedema over time
More infoSpectralis OCT Volume and line scans at follow up (left optic disc)
More info
Differential Diagnosis
Optic nerve head drusen
Small crowded discs
Tilted disc syndrome
Non-arteritic anterior ischaemic optic neuropathy (NAAION)
Artertic anterior ischaemic optic neuropathy (AAION)
Optic neuritis (papillitis)
Diabetic papillopathy
References
Arturo Carta, Stefania Favilla, Marco Prato, Stefania Bianchi-Marzoli, Alfredo A. Sadun, Paolo Mora; (2012) Accuracy of Funduscopy to Identify True Edema versus Pseudoedema of the Optic Disc. Invest. Ophthalmol. Vis. Sci. 2012;53(1):1-6.
Chiang, J., Wong, E., Whatham, A., Hennessy, M., Kalloniatis, M. and Zangerl, B. (2015), Differentiating optic nerve head swelling. Clin Exp Optom, 98: 12-24.
Mollan SP, Markey KA, Benzimra JD, et al (2014) A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertensionPractical Neurology14:380-390.
Rigi, M., Almarzouqi, S. J., Morgan, M. L., & Lee, A. G. (2015). Papilledema: epidemiology, etiology, and clinical management. Eye and brain, 7, 47–57.