
- Overview
- Patterns of Retinal Structure Loss
- RAPD in Retrograde Degeneration
- Case Examples
- Differential Diagnosis
- References
Overview
Cortical lesions may result in damage to the anatomically linked retinal nerve fibres in a process termed retrograde degeneration. This leads to sectoral or diffuse disc pallor with RNFL and ganglion cell thinning. Cupping of the disc can also occur in longstanding cases, hence retrograde degeneration is an important differential for glaucoma.
Retrograde degeneration can be classified as direct or trans-synaptic. Direct optic atrophy has a lot of overlap with primary optic atrophy.
On the other hand, trans-synaptic retrograde degeneration occurs when the lesion causing damage is located posterior to the lateral geniculate nucleus to (and including) the primary visual cortex.
Retro-chiasmal lesions cause a homonymous loss of the retinal ganglion cells on the contralateral (opposite) side to the lesion, and disc pallor on the ipsilateral (same) side. Anatomically, the reason for this is that at the chiasm, axons projecting from the nasal retina cross to the contralateral side of the brain. Thus, a lesion posterior to the chiasm will damage the temporal nerve fibres from the ipsilateral eye and the nasal fibres from the contralateral eye.
Retinal ganglion cell loss (seen in macular OCT scans) is preferred for identifying structural changes compared to optic nerve head scans. It is important to note however, that in some cases the visual field changes actually precede structural changes. Irrespective of the ocular findings, the gold standard for identifying the cause of retrograde degeneration remains neuroimaging.
Clinically, ganglion cell loss and the associated field loss both respect the vertical midline in retro-chiasmal retrograde degeneration. This is an important clinical feature that can help to differentiate RNFL loss due to retrograde from that other causes, particularly glaucoma which respects the horizonal midline rather than the vertical.
Patterns of Retinal Structure Loss
The pattern of retinal thinning in retrograde degeneration may predict the location of the cortical lesion causing the damage.
In brief:
- Lesions anterior to the chiasm produce monocular field loss only.
- Lesions at the chiasm cause a bitemporal visual field defect and bitemporal disc pallor.
- Retro-chiasmal lesions will cause homonymous field defects that affect the opposite half of the visual field. (eg. a defect posterior to the chiasm on the right side of the brain will cause a left homonymous field defect).
- Lesions affecting the lower bank of the optic radiations will cause a defect in the superior field, and upper bank lesions cause an inferior field defect.
- As a general rule, field defects due to occipital lobe lesions become more congruent the closer the lesion is to the occipital pole.
RAPD in Retrograde Degeneration
Only lesions anterior to the lateral geniculate nucleus (LGN) can have an RAPD.
Unilateral lesions anterior to the optic chiasm will cause an RAPD.
The presence of an RAPD relies on unequal visual input from the two eyes. Hence, a lesion at the optic chiasm will only cause an RAPD if the visual field of one eye is significantly more affected than the other.
A subtle RAPD may occur from retro-chaismal, pre-LGN lesions as 53% of nerve fibres cross at the chiasm meaning that the amount of information received at the LGN from the contralateral eye is slightly greater than that from the other eye. Hence, a lesion anterior to the LGN may cause a greater visual field loss in the contralateral eye (as compared to the ipsilateral eye), leading to a mild RAPD in the contralateral eye.
Case Examples
-
Case 1: Chiasmal lesion (early manifestation)
A 51 year old asymptomatic Caucasian male with best corrected visual acuities of 6/6 (20/20) in each eye.
Given the clinical findings shown below, this patient was referred promptly for a neurological assessment to exclude a compressive lesion at the optic chiasm.
-
Case 2: Pituitary tumour (advanced)
A 52 year old Caucasian male complaining of poor vision in the left eye for the last 3 years. His best corrected visual acuity is 6/7.5 (20/25) in the right eye and 6/75 (20/250) in the left.
Given the clinical findings below, this patient was referred urgently for a neurological assessment.
Fundus photographs (right and left eye)
More infoOptic disc photos (right and left eye)
More infoRed free posterior pole images (right and left eye)
More infoCirrus RNFL analysis
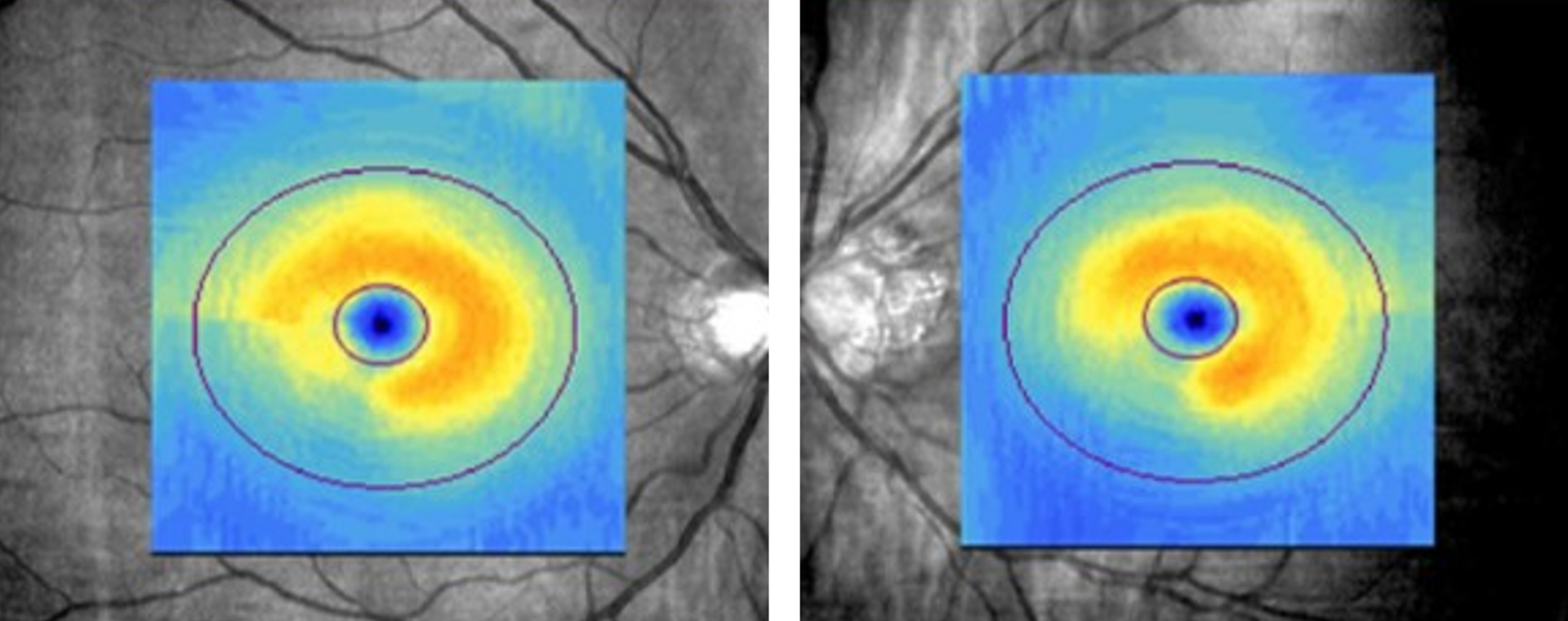
More infoCirrus Ganglion Cell Analysis
More infoCirrus PanoMap Analysis
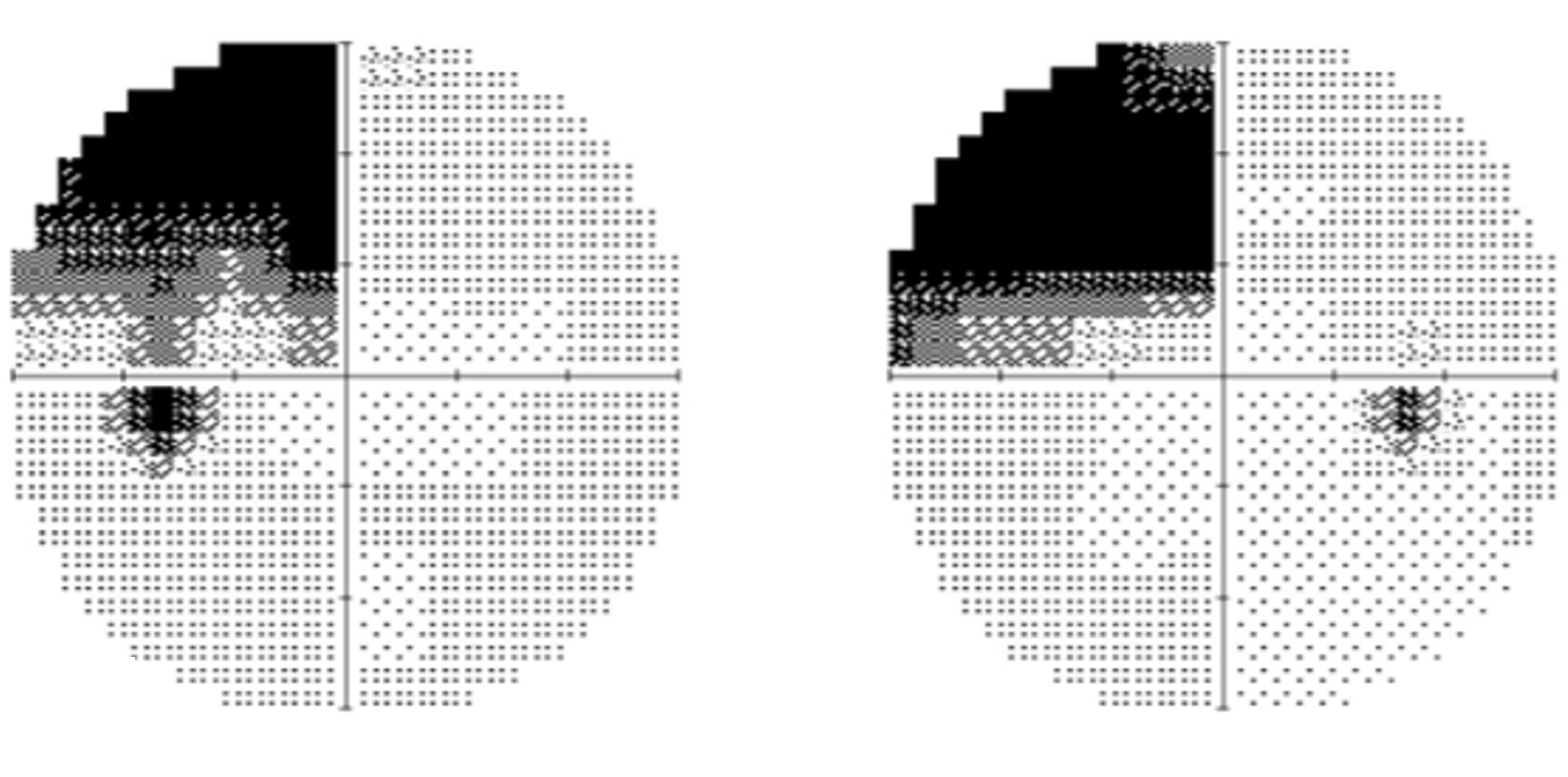
More info30-2 SITA-Fast visual field
More info -
Case 3: Left homonymous superior quadrantanopia (pie in the sky)
A 42 year old Asian female with best corrected visual acuity of 6/6- (20/20-) in each eye. No RAPD was present and the red cap test showed equal colour saturation between the two eyes. Additional neurological screening revealed reduced sensation on the left side of the face relative to the right.
Given the clinical presentation below, this patient was referred for prompt vascular and neurological work-ups.
-
Case 4: Right homonymous hemianopia
A 49 year old Asian male who has noticed recent difficulties reading. His best corrected visual acuity is 6/7.5 (20/25) in each eye. No RAPD is noted.
Given the clinical presentation below, this patient was referred promptly for neurological assessment to rule out a cortical lesion.
-
Case 5: Partial left homonymous hemianopia
A 57 year old Asian male who has a history of a traumatic brain injury from a car accident 6 years ago. His best corrected visual acuity is 6/7.5- (20/25-) in the right eye and 6/7.5-2 (20/25-2) in the left. NO RAPD was noted.
Given the patient history and clinical findings below, it was determined that the visual field defects noted were likely related to the traumatic brain injury.
Differential Diagnosis
References
Zangerl, B., Whatham, A., Kim, J., Choi, A., Assaad, N.N., Hennessy, M.P. and Kalloniatis, M. (2017), Reconciling visual field defects and retinal nerve fibre layer asymmetric patterns in retrograde degeneration: an extended case series. Clin Exp Optom, 100: 214-226.
Herro, A. M., & Lam, B. L. (2015). Retrograde degeneration of retinal ganglion cells in homonymous hemianopsia. Clinical ophthalmology (Auckland, N.Z.), 9, 1057–1064.