
Overview
Retinopathy of prematurity is a proliferative vitreoretinopathy occuring in people of premature birth (less than 31 weeks gestation), low birth weight (less than 1.25kg) or the use of supplemental oxygen after birth.
Retinal vasculature develops first at the posterior pole during gestation, with the peripheral vasculature developing over time. When babies are born prematurely, their retina has not yet been completely vascularised (with the temporal retina being the last quadrant of the retina to fully vascularise after birth). If a baby requires high-pressure ventilation after birth, this increased availability of oxygen (hyperoxia) inhibits the release of VEGF and therefore the development of the peripheral vasculature.
Once the supplemental oxygen is stopped, retinal hypoxia results as the vasculature has not developed sufficiently to meet the retina's metabolic needs. As a result, excessive VEGF is released, leading to neovascularisation. These vessels are fragile and supported by fibrovascular material that can contract over time, leading to the retinal changes seen in ROP, including "dragging" of the macula and tractional retinal detachment.
ROP is classified using the International Classification of Retinopathy of Prematurity (ICROP) into 5 stages, ranging from stage 1 (mildly abnormal blood vessel growth requiring no treatment) through to stage 5 (tractional retinal detachment and blindness). The classification system also considers the zones of the retina (1, 2, and 3) and the extent of the disease based on the clock hours.
Most ROP regresses spontaneously through a process of involution from a vasoproliferative stage to an involutional (previously termed 'cicatricial') stage.
Case Examples
-
Case 1
A 14-year-old male, born prematurely at 29 weeks. Visual acuity is 1/48-1 in each eye. He had strabismus surgery on his right eye at 2 years of age.
-
Case 2
A 19-year-old Asian female who was born prematurely at approximately 6 months gestation and spent several weeks in an incubator. Her best-corrected visual acuity is 6/7.6-1 (20/25-1) in each eye. Her right eye is highly myopic (-8.25DS) and her left less so (-3.75 /-2.00 x 60).
Fundus photographs (right and left eye)
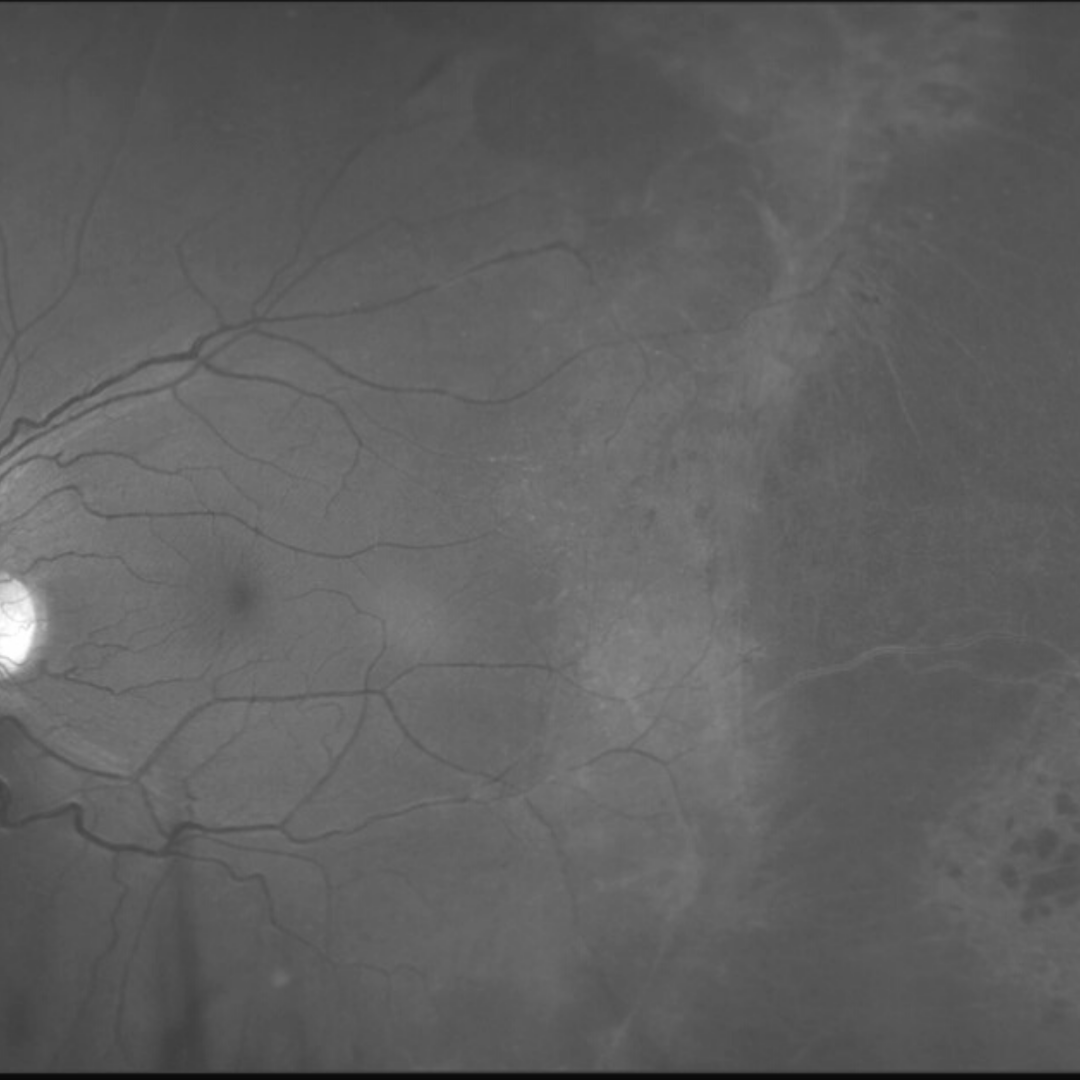
More infoRed free images (right and left eye)
More infoOptomap widefield and green separation image (right eye)
More infoOptomap widefield and green separation image (left eye)
More infoSpectralis OCT line scans (right eye, temporal retina)
More infoSpectralis OCT line scans (left eye temporal retina)
More info -
Case 3
A 32-year-old Middle Eastern male has had a right hyper-exotropia and poor vision in his right eye since he can remember. His visual acuity in the right eye is counting fingers at 2 metres and in the left eye is 6/9.5 (20/32). He was born prematurely at 30 weeks gestation.
Retinal photograph and red free image (right eye)
More infoRetinal photograph and red free image (left eye)
More infoOptomap and fundus auotofluorescence image (right eye)
More infoOptomap and fundus auotofluorescence image (left eye)
More infoGreen separation image (left eye)
More infoSpectralis OCT line scans (left temporal retina)
More infoSpectralis OCT macular line scan (left eye)
More info
Differential diagnosis
References
Chen, J., Smith, L.E.H. (2007) Retinopathy of prematurity. Angiogenesis 10, 133–140
Hellström,A., Smith,LEH., Dammann,O. (2013) Retinopathy of prematurity, The Lancet, Volume 382, Issue 9902, Pages 1445-1457,
International Committee for the Classification of Retinopathy of Prematurity. International Classification of Retinopathy of Prematurity (ICROP) Revisited. Arch Ophthalmol, 2005; 123: 991-999