
Overview
Branch retinal vein occlusion (BRVO) is a potentially sight-threatening condition due to the potential for the development of retinal neovascularisation and/or macular oedema. Population-based studies report a prevalence rate of between 0.5 - 2% for BRVO (Khayat et al. 2018).
Branch retinal vein occlusions are thought to occur when thickening of the arteriole sharing its sheath leads to compression causing an increase in the intraluminal pressure. This in turn results in transudation of blood, protein and associated products into the surrounding retina as well as increasing the intestitial pressure, causing retinal odema and in some cases retinal ischaemia.
In response to ischaemia, vascular endothelial growth factor (VEGF) is released by the retina which may stimulate the growth of new vessels attempting to normalize blood flow to the ischaemic retina.
Case Examples
-
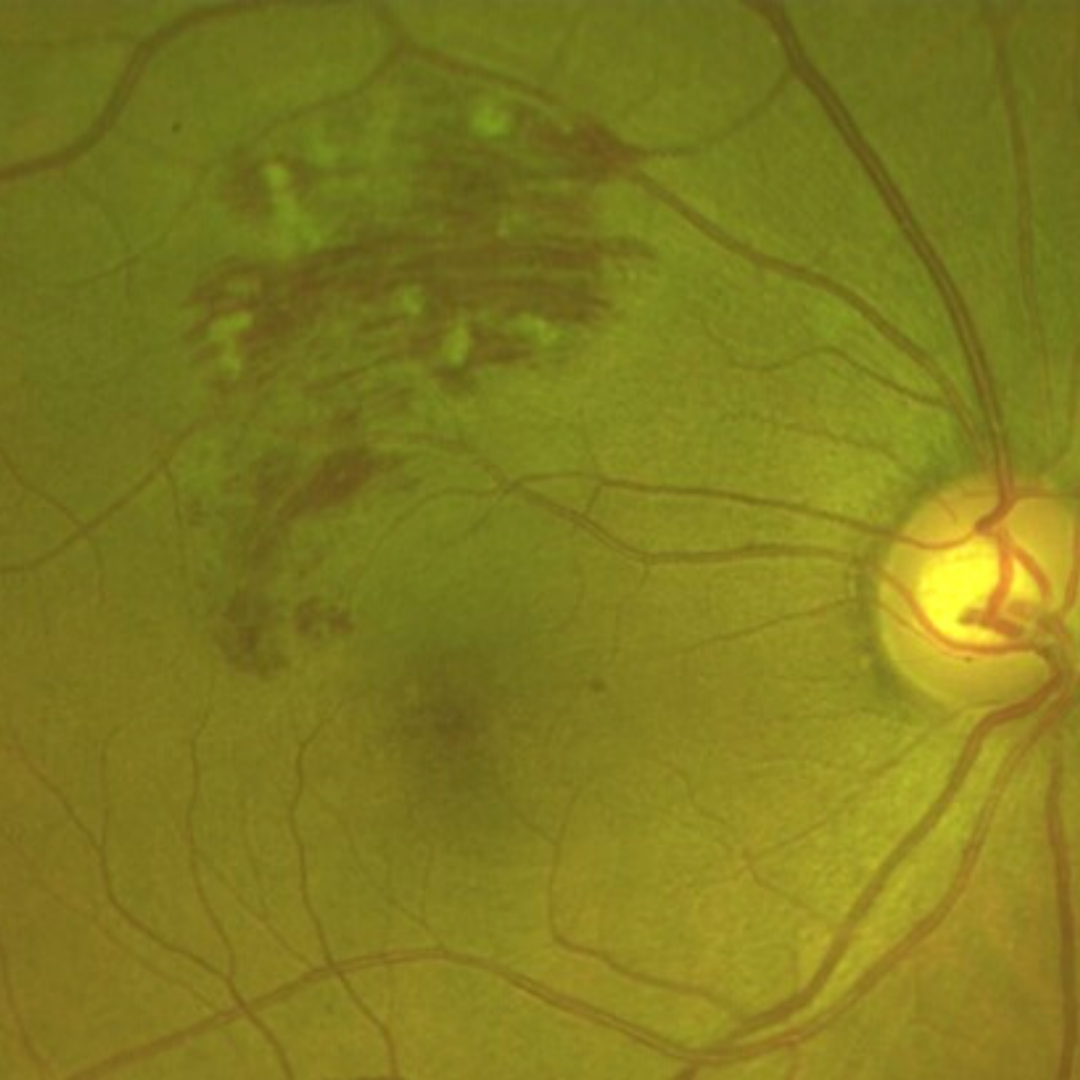
Case 1: Acute BRVO
A 58 year old Asian female with best corrected visual acuity of 6/6- (20/20-) in the right eye.
-
Case 2: Chronic BRVO
A 69 year old Asian male with a history of branch retinal vein occlusion in his left eye, diagnosed 9 months previously. His best corrected visual acuity was 6/6 (20/20) in this eye and his intraocular pressures 11mmHg in both eyes.
-
Case 3: Chronic BRVO with collateral vessels
A 72 year old Caucasian female with best corrected visual acuity in this eye of 6/19+. Testing with an Amsler grid revealed no metamorphopsia and intraocular pressures were 18mmHg in both eyes. She has a history of branch retinal vein occlusion.
-
Case 4: Chronic, treated BRVO
A 69 year old Asian male with untreated hypertension (blood pressure in office 158/98). His best corrected visual acuity in each eye was 6/6- and intraocular pressures 20mmHg (OD) and 22mmHg (OS).
Fundus photograph and red-free image (right eye)
More infoFundus photograph and red-free image (left eye)
More infoOptomap and green separation image (right eye)
More infoOptomap and green separation image (Left temporal retina)
More infoSpectralis OCT line scan (left eye)
More infoSpectralis OCT volume scan (left temporal retina)
More info
Differential Diagnosis
References
Jia Li, Yannis M. Paulus, Yuanlu Shuai, Wangyi Fang, Qinghuai Liu, and Songtao Yuan (2017) New Developments in the Classification, Pathogenesis, Risk Factors, Natural History, and Treatment of Branch Retinal Vein Occlusion. Journal of Ophthalmology Volume 2017 |Article ID 4936924.
Khayat, Survey Ophth 2018. Major Review: Ischemic retinal vein occlusion: characterising the more severe spectrum of retinal vein occlusion
Patel, A., Nguyen, C., & Lu, S. (2016). Central Retinal Vein Occlusion: A Review of Current Evidence-based Treatment Options. Middle East African journal of ophthalmology, 23(1), 44–48.
Woo SCY , Eye 2016. Associations of RAO and RVO to mortality, stroke and myocardial infarction: a systematic review