
Overview
Retinal vein occlusions can lead to an increase in intraluminal venous pressure which causes capillary endothelial cell damage and capillary dropout. The resultant ischaemia causes an upregulation of vascular endothelial growth factor (VEGF) which stimulates the development of new vessels (neovascularisation). These new vessels may be found at the disc (NVD), elsewhere in the retina (NVE) and/or on the iris (NVI). A major factor in the development of neovascularisation in retinal vein occlusions is the severity and extent of retinal ischaemia.
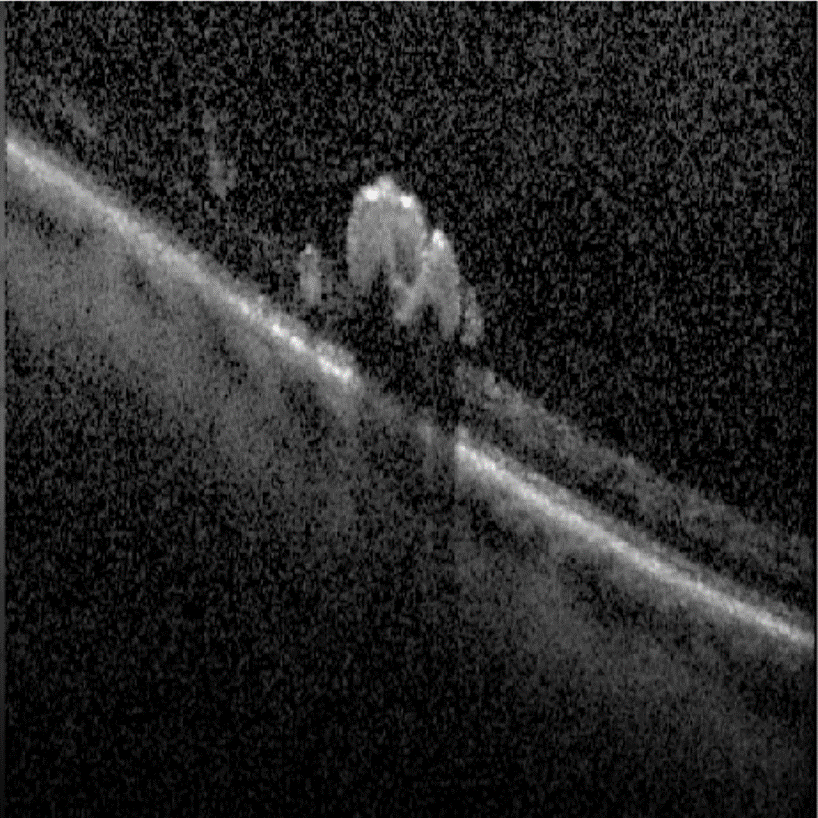
Retinal neovascularisation first develops within the retina but can breach the internal limiting membrane (ILM) and progress into the vitreous cavity. On OCT imaging, hyper-reflective lesions can be seen on the retinal surface and may attach to the posterior hyaloid. OCT-angiography can be used to confirm the presence of neovascularisation by showing a hyper-reflective network within the vitreoretinal interface.
In BRVO, the major site of neovascularisation is the retina or at the optic disc while CRVO have a higher risk of iris neovascularisation and subsequent neovascular glaucoma. The majority of neovascular glaucoma presents within 3 months of the initial event and is sometimes refer '90-day glaucoma'.
Ocular neovascularisation is the most common within the first 6-12 months following a retinal vein occlusion, however it can occur up to 3 years after. Therefore, regular comprehensive assessments are required for all cases of retinal vein occlusions. This should include slit lamp examination and gonioscopy to detect neovascularisation of the iris and/or angle, as well as dilated fundus examinations.
Rubeosis Irides
-
Case 1
A 75 year old Caucasian female. Intraocular pressures are 12mmHg in the right eye and 48mmHg in the left. The vision in her left eye is light perception only.
-
Case 2
A 75 year old Asian male. Vision in the right eye recorded as no light perception. He reports that the eye has been blind for a few years.
Retinal Neovascularisation
-
Case 1
A 62 year old Asian male with a history of BRVO in his right eye that was treated with panretinal laser photocoagulation 6 years ago. The best corrected visual acuity is 6/4.8 (20/15) in the right eye.
Fundus photograph and red-free image (right eye)
More infoOptomap and green separation images (right eye)
More infoFundus autofluorescence imaging (right eye)
More infoSpectralis OCT volume scan (right supero-temporal retina)
More infoSpectralis OCT line scans through area of neovascularisation
More infoOCT Angiography through area of neovascularisation
More info
Differential Diagnosis
References
Khayat, Survey Ophth 2018. Major Review: Ischemic retinal vein occlusion: characterising the more severe spectrum of retinal vein occlusion
Patel, A., Nguyen, C., & Lu, S. (2016). Central Retinal Vein Occlusion: A Review of Current Evidence-based Treatment Options. Middle East African journal of ophthalmology, 23(1), 44–48.
Sohan Singh Hayreh, Patricio Rojas, Patricia Podhajsky, Paul Montague, Robert F. Woolson (1983) Ocular Neovascularization with Retinal Vascular Occlusion-III: Incidence of Ocular Neovascularization with Retinal Vein Occlusion, Ophthalmology, Volume 90, Issue 5.