
Overview
Sickle cell retinopathy results from a mutant gene that codes for the amino acids contained in haemoglobin. This causes the red blood cells to deform into a “sickle”shape when oxygen pressure is low. Retinal changes occur secondary to vaso-occlusion and local ischemia. Sickle cell retinopathy is most prevalent in the African American population.
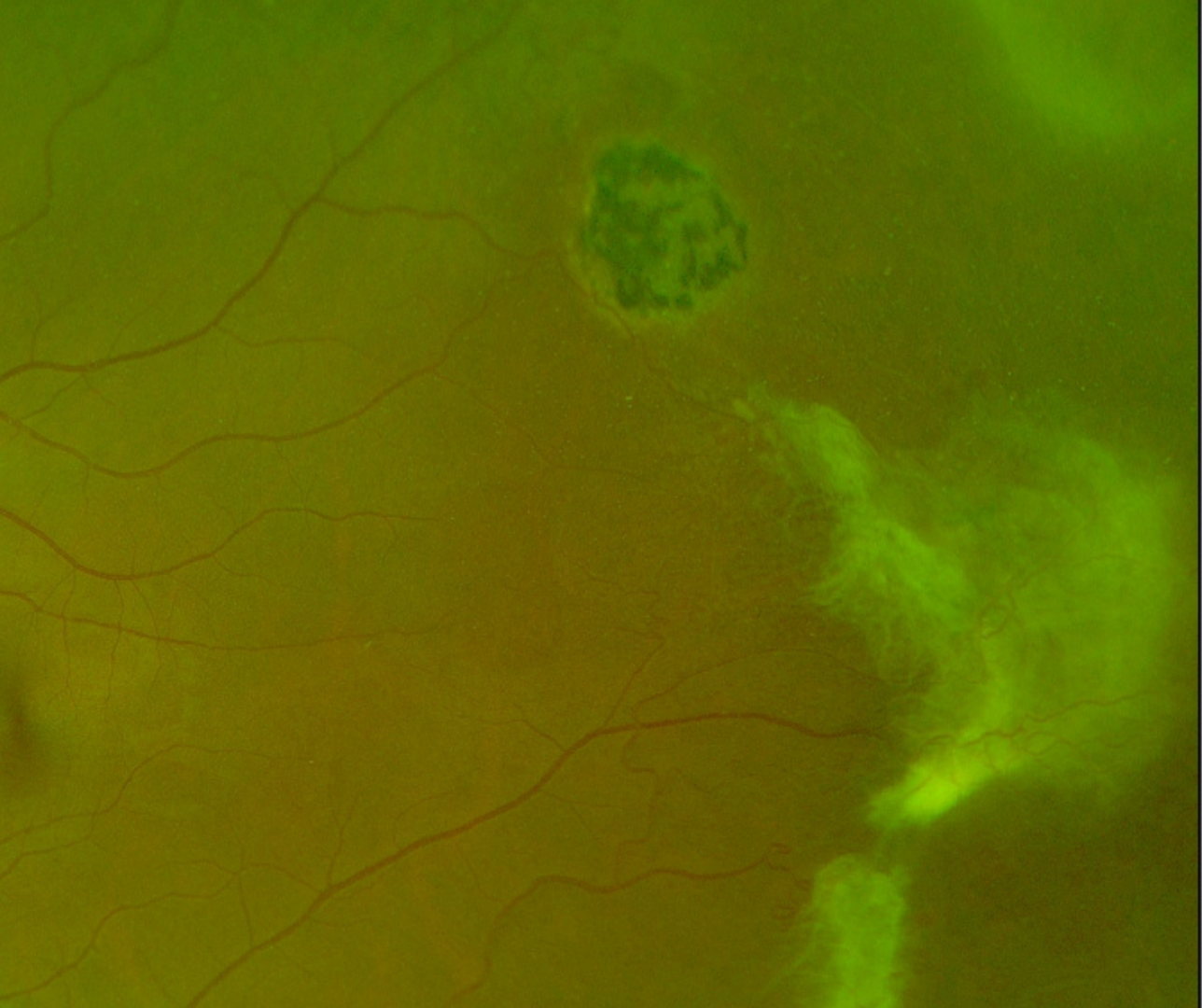
Sunburst lesions are localized areas of retinal pigment hypertrophy, hyperplasia and pigment migration as seen in the OCT. The lesions often appear speculated and are typically found in the peripheral retina in a perivascular location. The ”sunburst” lesions usually form secondary to reabsorbed sub-retinal haemorrhages and appear on fundus autofluorescence as an area of hypo-autofluorescence with a hyper-autofluorescent border. They are characteristic of sickle-cell retinopathy.
Decreased visual acuity occurs due to the occlusion of parafoveal capillaries and arterioles, as well as spontaneous occlusion of the central retinal artery in some patients.
This patient also has a second characteristic feature of sickle cell retinopathy – pre-retinal “sea fan” neovascularization. This typically occurs in sickle-cell patients at the posterior border of an area of retinal non-perfusion, and can lead to vitreous haemorrhage and eventually tractional retinal detachment.
Other possible clinical findings typical of sickle cell retinopathy include the segmentation of blood in the blood vessels of the conjunctiva or the small surface vessels of the optic disc.
Case Examples
-
Case 1: Sickle cell retinopathy
A 26 year old African female with best corrected visual acuity of 6/7.5- (20/25) in each eye. Her medical history included a diagnosis of sickle cell disease.
Optomap widefield images (right eye)
More infoOptomap green separation image (right eye)
More infoOptomap widefield images (left eye)
More infoOptomap widefield images (left eye)
More infoFundus autofluorescence images (right eye - top, left eye - bottom)
More infoSpectralis OCT macular line scans (right eye - top, left eye - bottom)
More infoSpectralis OCT line scans (taken through the infero-temporal peripheral lesion, right eye)
More infoSpectralis OCT line scans (1 - taken through the white lesion in the temporal retina, 2 - taken through the hyper-pigmented supero-temporal lesion)
More info -
Case 2: Sickle cell retinopathy
A 27 year old African male who has been diagnosed with sickle cell disease.
Optomap (1), green separation (2) and fundus autofluroescence (3) images - right eye
More infoOptomap (1), green separation (2) and fundus autofluroescence (3) images - left eye
More infoSpectralis OCT volume and line scans (right macula)
More infoSpectralis OCT volume and line scans (left macula)
More infoCirrus ganglion cell analysis
More info -
Case 3: Proliferative sickle cell retinopathy
A 45 year old female diagnosed with sickle cell disease 14 years previously. Current smoker. Otherwise healthy.
Colour fundus photographs
More infoOptomap widefield imaging (right eye, supero-temporal retina)
More infoOptomap widefield imaging (temporal retina, left eye)
More infoSpectralis OCT line scan (left eye, temporal retina)
More infoSpectralis OCT line scan (right eye, superior-temporal retina)
More infoSpectralis OCT line scan (A), OCT angiography superficial vascularu plexus (B); Cirrus macular thickness map (C and D). All images are the right eye.
More info
Differential Diagnosis
References
Abdalla Elsayed, M.E.A., Mura, M., Al Dhibi, H. et al. (2019) Sickle cell retinopathy. A focused review. Graefes Arch Clin Exp Ophthalmol 257, 1353–1364.
Menaa, F., Khan, B. A., Uzair, B., & Menaa, A. (2017). Sickle cell retinopathy: improving care with a multidisciplinary approach. Journal of multidisciplinary healthcare, 10, 335–346.