
Overview
Choroideraemia is an X-linked condition affecting the RPE, outer retina, and choriocapillaris. It is caused by mutations in the CHM gene. Due to this inheritance pattern, choroideraemia is much more common in males than in females.
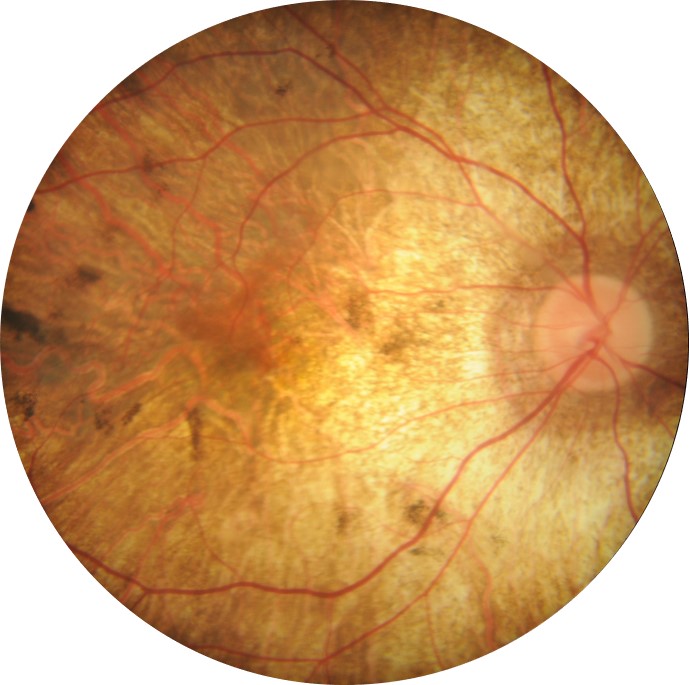
The disease process is characterised by nyctalopia and peripheral vision loss in the second decade of life or before. In the early stages, peripheral pigmentary mottling may be noted and over time this develops into pigment clumping and atrophy of the RPE, photoreceptors, choriocapillaris and eventually, choroidal atrophy follows.
Over time, loss of the RPE means that the choroidal vasculature becomes more visible. As the disease progresses and further atrophy of the choroid occurs (usually in the mid-peripheral and peripapillary fundus first) and the bare sclera may become visible – seen clinically as areas of pale white areas on retinal imaging.
Pigment clumping occurs as a result of RPE degeneration. This pigment can be seen on OCT as hyper-reflective deposits. Also seen on OCT are interlaminar bridges (ILBs) which are hypo-reflective wedge-shaped structures that bridge the inner and outer retina in choroideraemia. Outer retinal tubulations are seen in late-stage disease on OCT. These appear as hyper-reflective round structures with a hypo-reflective lumen. The tubulations are composed of deteriorating photoreceptors and remnants of the external limiting membrane.
In recent studies, OCT angiography has been used to further our knowledge around choroideraemia. These studies showed that the choriocapillaris shows greater nonperfusion than the retina in choroideraemia.
Disease progression is relatively slow with central vision being fairly well preserved until late stage disease starts to affect the macula – typically around 50 to 70 years of age.
Being an x-linked condition, females are rarely diagnosed with choroideraemia, however the carriers of the defective gene may show a partial expression of the condition. Most carriers are asymptomatic and visual acuity is unaffected, however the fundus may show signs consistent with choroideraemia such as pigment mottling.
Case Examples
-
Case 1: Choroideraemia
A 42-year-old caucasian male with best-corrected visual acuity of 6/9.5 (20/30) in the right eye and 6/12 (20/40) in the left.
Posterior pole photos (right and left eye)
More infoOptomap (top) and green separation (bottom) images - right eye
More infoOptomap (top) and green separation (bottom) images - left eye
More infoFundus autofluorescence imaging (right and left eye)
More infoSpectralis OCT volume and line scans - right macula
More infoSpectralis OCT volume and line scans - left macula
More info10-2 SITA standard visual field
More info -
Case 2: Advanced choroideraemia complicated by macular oedema
A 72-year-old Caucasian male with best-corrected visual acuity of 6/12+ (20/40+) and 6/38 (6/127) in the left eye. He reports longstanding night vision difficulties and poor peripheral vision.
Posterior pole photos (right and left eye)
More infoOptomap and green separation images (right eye)
More infoOptomap and green separation images (left eye)
More infoSpectralis OCT volume scan (right macula)
More infoSpectralis OCT line scan (left macula)
More infoSpectralis OCT volume scan (left macula)
More info -
Case 3: Choroideraemia carrier
A 34-year-old Caucasian female with best-corrected visual acuity of 6/6 (20/20) in each eye. Her father has been diagnosed with choroideraemia.
Optomap (1) red separation (2) and green separation (3) images - right eye
More infoOptomap (1) red separation (2) and green separation (3) images - left eye
More infoFundus autofluorescence images (right and left eye)
More infoSpectralis OCT line scans (right and left eye)
More infoElectrophysiology results
More info -
Case 4: Choroideraemia carrier
A 55-year-old female with best-corrected visual acuity of 6/6 (20/20) in each eye. The patient's father had choroideraemia and was legally blind at age 40. She reports no difficulty with night vision.
Colour fundus photographs (right and left eye)
More infoOptomap (1), red separation (2) and green separation (3) images - right eye
More infoOptomap (1), red separation (2) and green separation (3) images - left eye
More infoFundus autofluorescence imaging (right and left eye)
More infoSpectralis OCT volume (1) and line (2) scans - right macula
More infoSpectralis OCT volume (1) and line (2) scans - left macula
More info
Differential Diagnosis
References
MacDonald, IM. Russell, L. Chan, CC (2009) Choroideremia: New Findings from Ocular Pathology and Review of Recent Literature, Survey of Ophthalmology, Volume 54, Issue 3, Pages 401-407.
Sun, LW, Johnson, RD, Williams, V. Summerfelt, P. Dubra, A. Weinberg, DV, Stepien, KE, Fishman, GA, Carroll, J. (2016). Multimodal Imaging of Photoreceptor Structure in Choroideremia. PLoS One, 11(12)
Zinkernagel, MS. & MacLaren, RE. (2015). Recent advances and future prospects in choroideremia. Clinical Ophthalmology, 9, 2195-2200.