
Overview
Posterior vitreous detachment (PVD) occurs in the majority of people as they age with a prevalence of 89% in the age range of 80-89 years.
The vitreous is attached to the retina at several places in the eye with the strongest attachments at the vitreous base and margins of the optic disc. Other attachments exist at the macula and posterior lens surface and there are weak attachments along the superficial retinal vessels.
Additional areas of strong or abnormal vitreous attachments can also exist (links available at the bottom of the page).
The major components of the vitreous humor include collagen fibres (~0.5%), hyaluronic acid (~0.5%) and water, which constitutes approximate 99% of the volume. Over time the vitreous gel undergoes a process of liquefaction (synchysis) and collagen fibrils aggregate into bundles (syneresis). As liquefaction increases, there is a gradual separation between the posterior vitreous cortex and the internal limiting membrane of the retina.
As the PVD progresses, areas of abnormally strong vitreoretinal attachments may be associated with retinal hole or tear formation. Operculated and horse-shoe tears are discussed elsewhere in the atlas (link below). Retinal tears have been found to be more common in patients who have retinal or vitreal haemorrhage associated with a PVD, and those with a higher frequency of floaters.
A rhegmatogenous retinal detachment will only occur if the vitreous is liquefied to some degree and there is some traction present.
Clinical Signs
Patients with PVD will often present with associated symptoms including sudden-onset floaters or flashes in the visual field. The flashes are believed to be due to retinal traction while the floaters are due to light passing through a collapsing vitreous and aggregated collagen fibres.
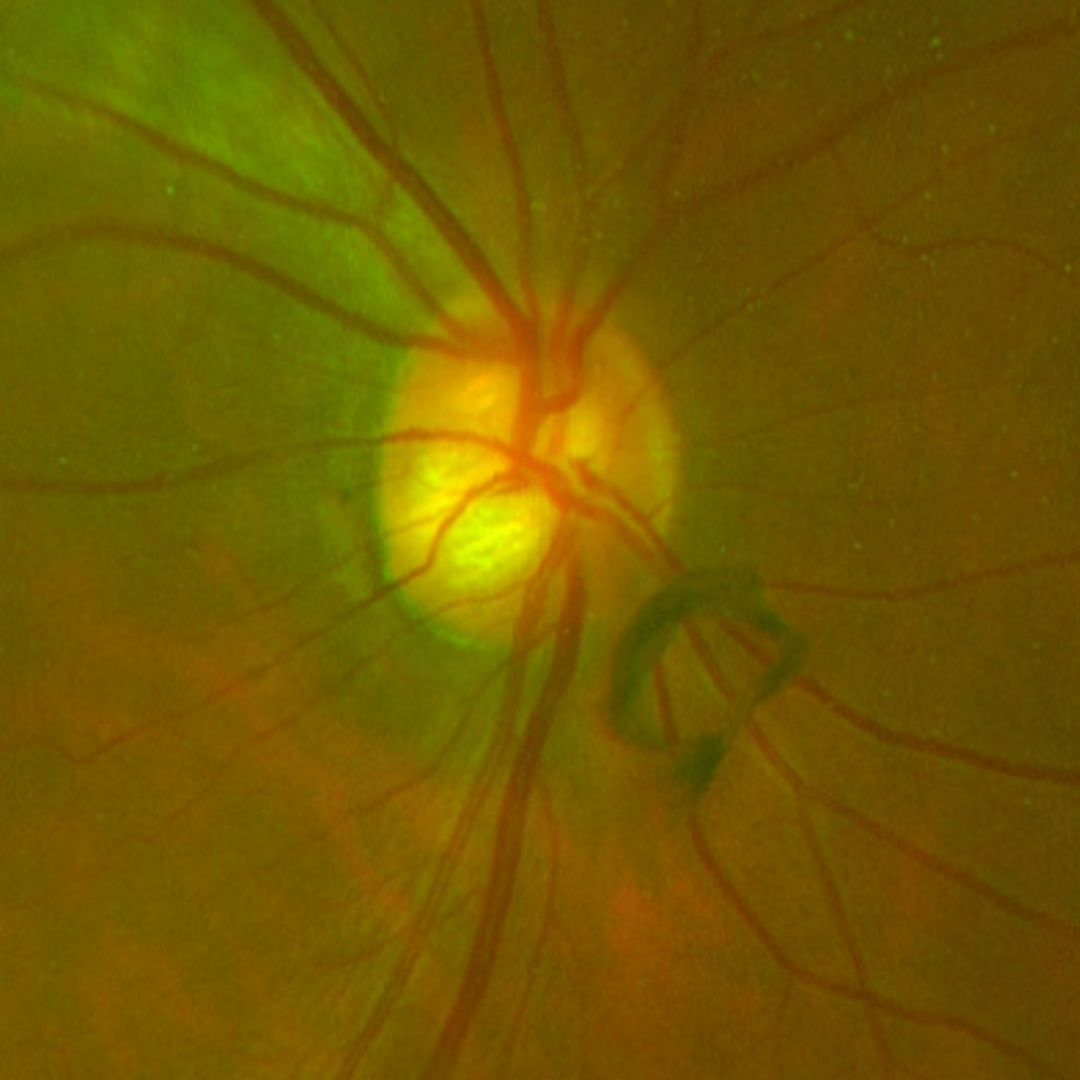
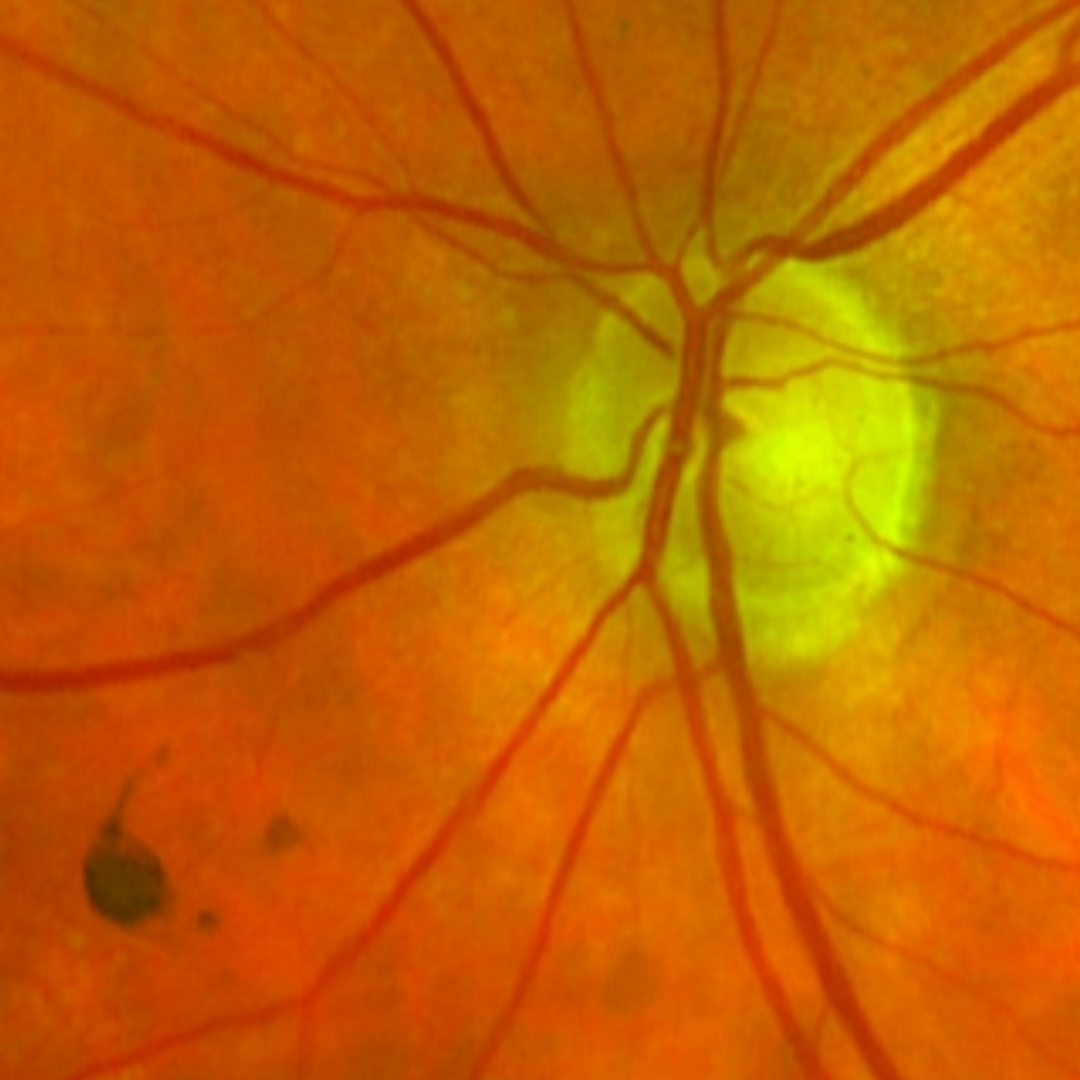
On fundoscopy, a dark floater may be seen at the posterior pole (Weiss ring) and, on OCT, complete separation of the vitreous cortex from the inner limiting membrane may be noted.
The term “complicated” PVD refers to a presentation where the vitreous base has detached in some areas however there are still areas of persistent vitreoretinal attachment.
PVD usually occurs in the other eye within 6 months to 2 years after the first eye.
References
Bond-Taylor, M., Jakobsson, G., & Zetterberg, M. (2017). Posterior vitreous detachment - prevalence of and risk factors for retinal tears. Clinical ophthalmology (Auckland, N.Z.), 11, 1689–1695.
Ghazi, N., Green, W. Pathology and pathogenesis of retinal detachment. Eye 16, 411–421 (2002).
Schweitzer KD, Eneh AA, Hurst J, Bona MD, Rahim KJ, Sharma S. (2011) Predicting retinal tears in posterior vitreous detachment. Can J Ophthalmol. Dec;46(6):481-5.