
- Overview
- Clinical Presentation
- Risk Factors
- Prognosis
- Case Examples
- Lesions Pre-Disposing to RRD
- Differential Diagnosis
- References
Overview
Retinal detachment is a condition whereby the neurosensory retina is separated from the retinal pigment epithelium (RPE). There are three types of retinal detachment, categorised according to the underlying mechanism – exudative, tractional and rhegmatogenous. The first two will be explored elsewhere in this atlas and this section will concentrate on rhegmatogenous retinal detachment (RRD).
A RRD occurs when there is a break in the retina (hole or tear) which allows fluid to enter the sub-retinal space and separate the neurosensory retina and the RPE. Patients with RRD typically present with the perception of light flashes, floaters, or a dark "curtain" over their vision however retinal detachments may also be detected during routine examination in asymptomatic patients.
Clinical Presentation
Retinal detachment gives the retina a semi-transparent appearance on funduscopy and this can become more opaque over time. Underlying choroidal detail may be obscured. The detachment of the neurosensory retina also gives it a wrinkled appearance (in contrast to a retinoschisis that has a smooth, translucent appearance). An associated retinal break (hole or tear) is seen in RRD.
Chronic retinal detachments show a pigmented demarcation line at the edge of the detachment. The affected retina may show whitish folds and intraretinal exudates.
Peripheral OCT imaging can be used to confirm the separation of the photoreceptors from the RPE. The associated retinal break may be seen on OCT as a full thickness break. This initial break allows fluid the opportunity to enter the potential space between the neurosensory retina and the RPE, pushing the two layers apart. Chronic retinal detachments may be associated with retinal cyst formation and RPE hyperplasia.
Visual fields show a relative scotoma corresponding to the area of retina that has been detached. This differs from the absolute scotoma associated with a retinoschisis.
The term "Shafer's sign" refers to the presence of pigment cells in the vitreous and may be seen in cases of retinal tear, RRD or a history of intraocular surgery. The presence of pigment is a strong indicator of a retinal break and further investigation is essential.
Risk Factors
Established risk factors for retinal detachment include posterior vitreous detachment, high myopia, lattice degeneration, cataract surgery, trauma, family history of retinal detachments in a first-degree relative and RRD in the fellow eye. Other conditions with an increased risk of retinal detachment include retinopathy of prematurity and Stickler syndrome.
Prognosis
An early diagnosis of RRD is vital. The visual prognosis is much improved if a RRD is treated before the macula becomes involved. Once the macula has been detached however, the prognosis is more guarded.
Some studies have shown no difference in visual outcome if a macula-off detachment is repaired anytime within 1 week of occurrence, however a recent study (Greven et al. 2019) showed significant differences in final visual acuity between patients whose macula-off detachments were treated within 1 day when compared with those treated within 3 days. The authors concluded that this type of detachment should be treated as soon as possible after diagnosis.
Frings et al. (2016) also showed that treatment of a macula-off detachment after 10 days produces a clinically comparable outcome to surgery undertaken up to 30 days post-macular-off detachment.
When assessing retinal breaks with regards to urgency of referral, it is helpful to keep the following general guidelines in mind:
- All acute retinal detachments require urgent referral.
- A pigmented demarcation line indicates chronicity of a retinal detachment.
- Symptomatic retinal breaks are more likely to progress to retinal detachment than non-symptomatic breaks.
- A superior retinal detachment is more likely to progress than an inferior one, due to the effects of gravity. Inferior detachments are typically slowly progressive, if at all, and may self-seal over time with no intervention.
- A horseshoe retinal tear and traumatic retinal breaks (e.g. retinal dialysis) are highly likely to progress and require urgent treatment.
- Atrophic and operculated retinal breaks are associated with a low risk of progression to RRD.
Case Examples
-
Case 1: Macula-on detachment
A 60-year-old Caucasian female has noted a recent onset of floaters in her right eye. She reports no history of trauma. Her best corrected visual acuity in this eye is 6/9 (20/30).
Given the clinical findings below, this patient was referred urgently for treatment of a macula-on retinal detachment.
-
Case 2: Macula-on detachment
A 22-year-old Asian female who noticed an increase in floaters in her left eye several weeks previously after being struck on the head. She is a high myope.
Given the superior nature of the detachment and ocular history, this patient was given an urgent referral to an ophthalmologist for assessment.
-
Case 3: Macula-off detachment
A 48-year-old South American female presented with a 2-month history flashes and floaters with a subsequent black patch in her vision from her left eye. She has a history of amblyopia in that eye but notes that her vision is significantly worse than before.
Pinhole acuity in the left eye was 6/120 (20/400-) and the left pupil was found to be unreactive.
Given the clinical appearance and ocular history, this patient was referred to an ophthalmologist for reattachment surgery.
-
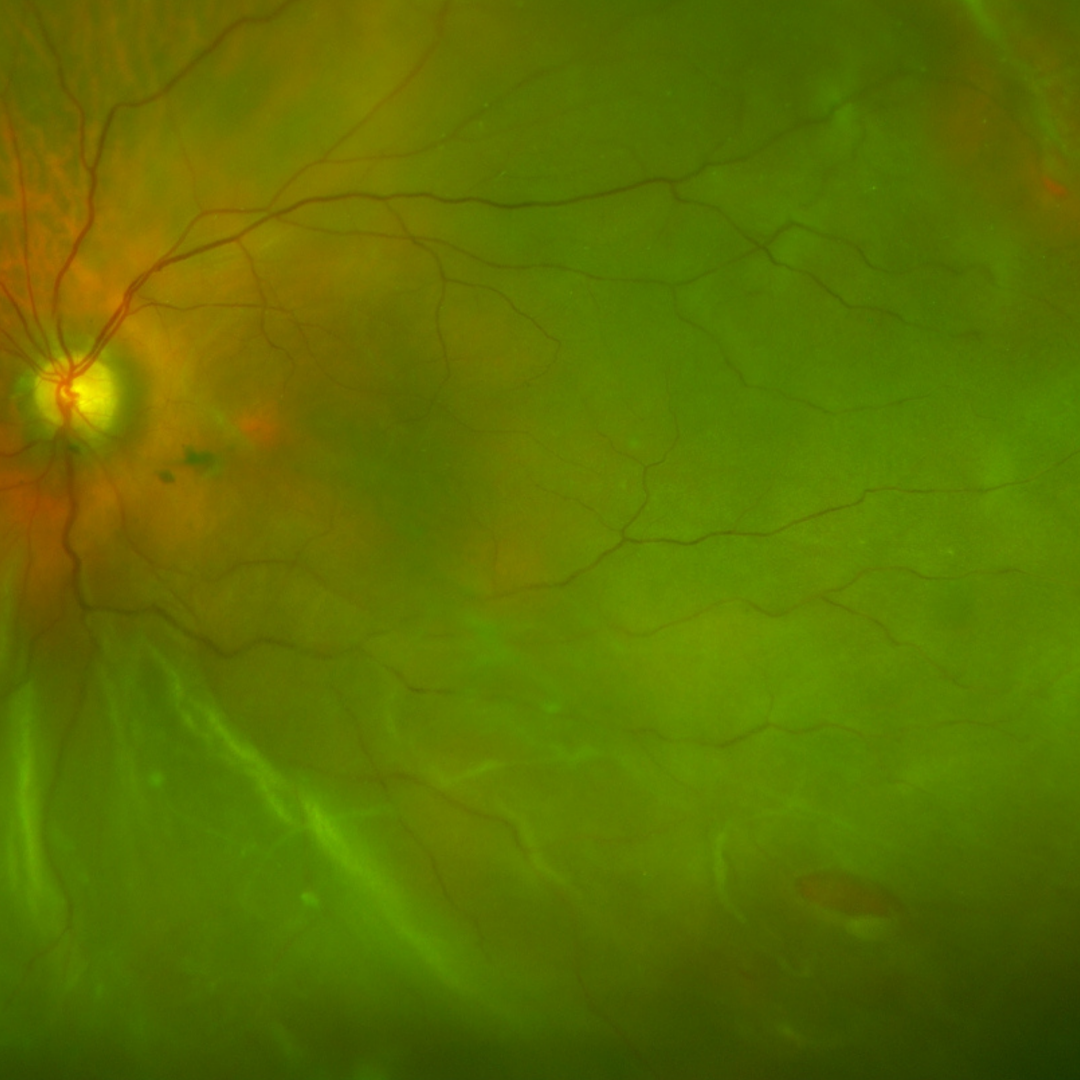
Case 4: Subtle retinal detachment
A 30-year-old asymptomatic Caucasian male with best corrected visual acuity of 6/6 (20/20) in the left eye.
-
Case 5: Long-standing macula-off retinal detachment
A 28 year old highly myopic Asian male with a history of visual symptoms and subsequent reduced vision 12 months ago in the left eye. Best corrected visual acuity in the left eye was 6/95+ (20/316+), achieved using eccentric fixation.
-
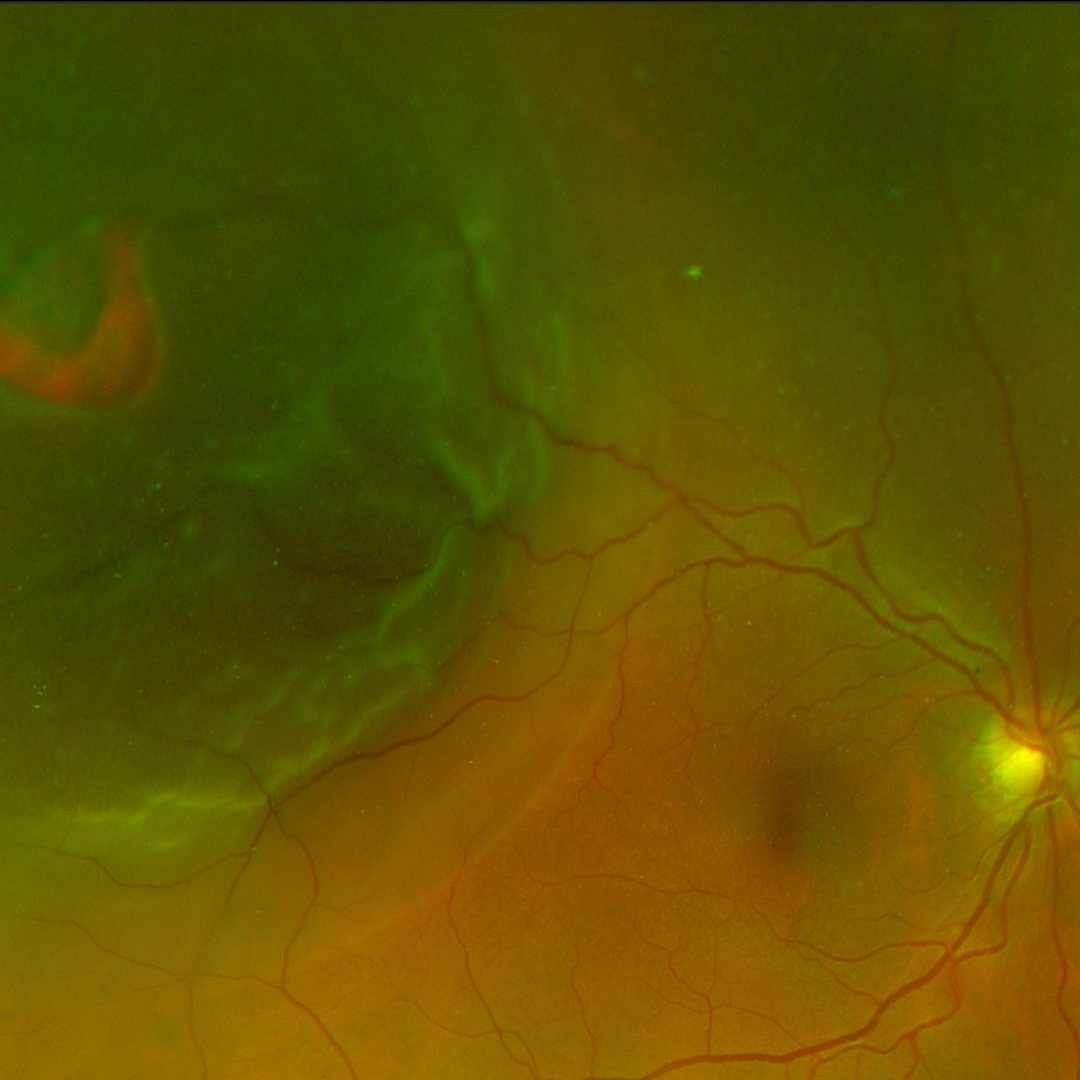
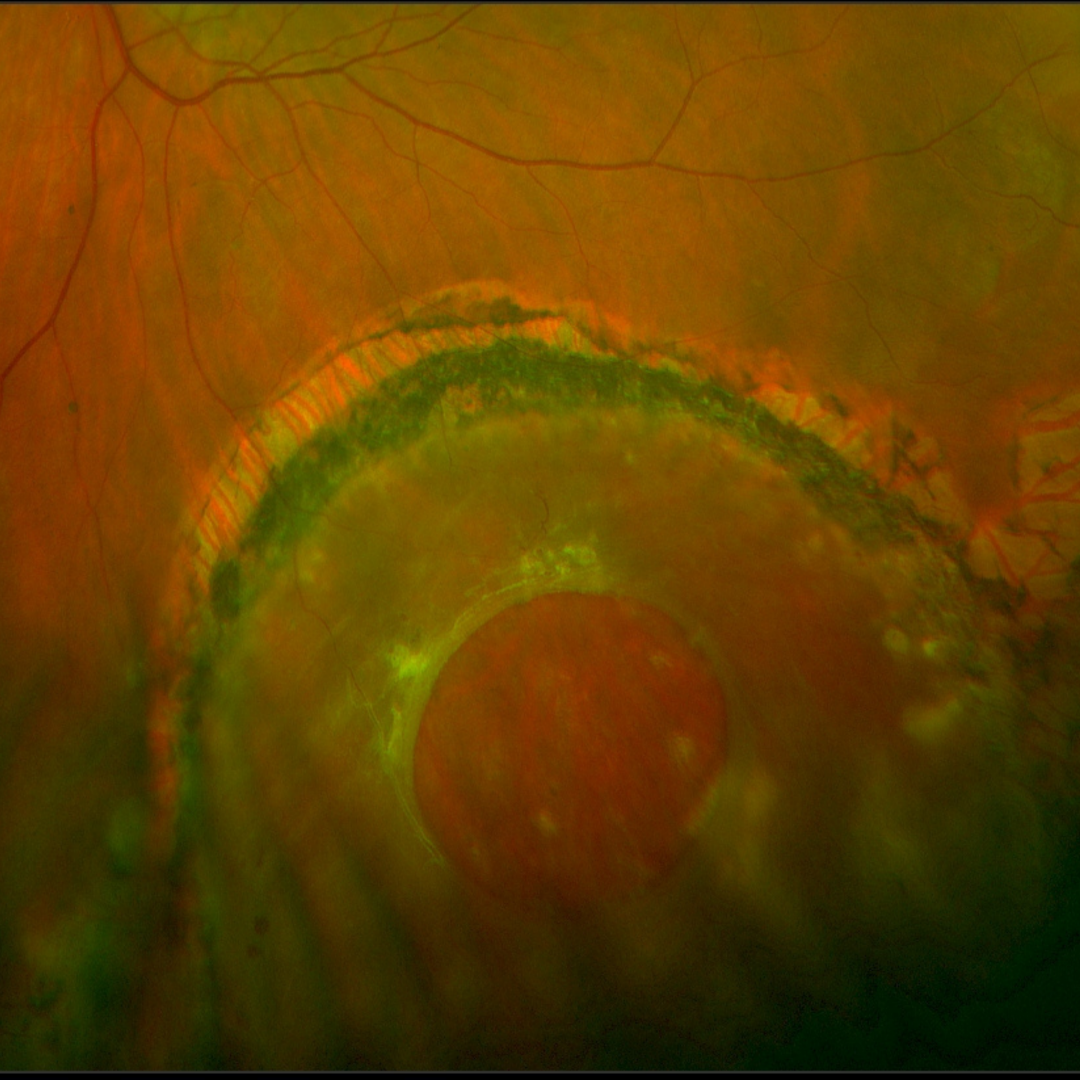
Case 6: Chronic retinal detachment
An asymptomatic 51-year-old Asian male with high myopia and best corrected visual acuity of 6/30-1 (20/100-1) in the right eye and 6/6 (20/20) in the left eye.
Given the chronic nature of the retinal detachments, they are unlikely to require treatment, however this patient was referred to an ophthalmologist for assessment.
Optomap pseudocolour (top) and green separation (bottom) images - right eye
More infoOptomap pseudocolour (top) and green separation (bottom) images - left eye
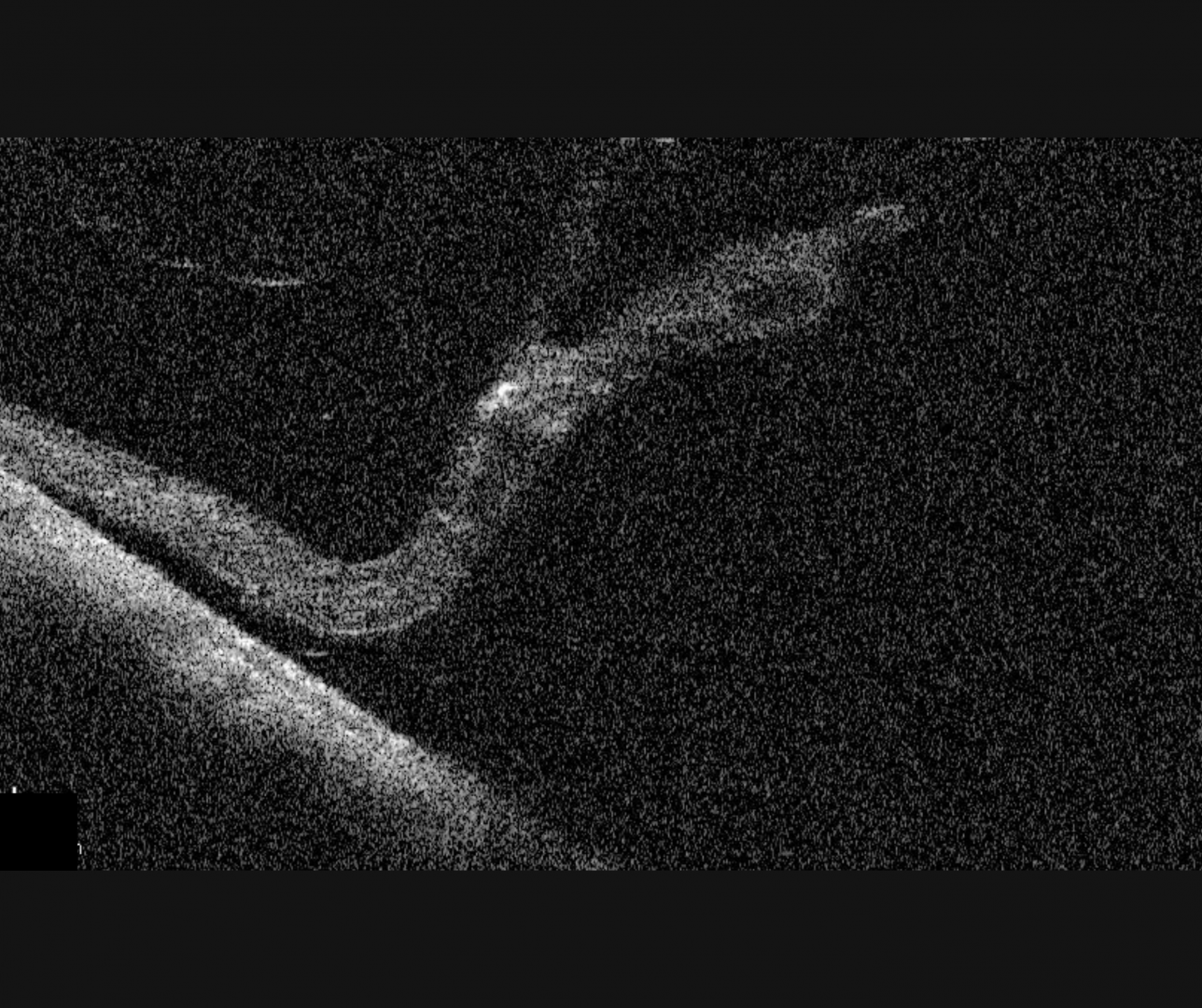
More infoSpectralis OCT line scans through the area of chronic detachment (right eye)
More infoSpectralis OCT volume scan through the area of chronic detachment (right eye)
More info -
Case 7: Self-sealed retinal detachment
An asymptomatic 53-year-old Caucasian male with a history of blunt trauma to the left eye at 7 years of age. His best corrected visual acuity was 6/7.5 (20/25) in the left eye. There is no history of past laser treatment.
Lesions Pre-Disposing to RRD
Differential Diagnosis
References
Frings A, Markau N, Katz T, et al (2016) Visual recovery after retinal detachment with macula-off: is surgery within the first 72 h better than after? British Journal of Ophthalmology 100:1466-1469.
Greven MA, Leng T, Silva RA, et al (2019) Reductions in final visual acuity occur even within the first 3 days after a macula-off retinal detachment. British Journal of Ophthalmology 103:1503-1506.
H. Dunbar Hoskins Jr., MD Center for Quality Eye Care (2019) Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern. American Academy of Ophthalmology.
Wilkinson,C. and Cochrane Eyes and Vision Group Cochrane Database Syst Rev. (2014) Sep; 2014(9): CD003170.