
Overview
Patients with uveitis have approximately 20% chance of developing glaucoma. The mechanisms underpinning glaucoma in uveitis are complex, and may include both open angle and angle closure mechanisms.
Open angle glaucoma may arise due to the mechanical obstruction of the trabecular meshwork by debris such as inflammatory cells and protein. Inflammation of the trabecular meshwork and aqueous hyper-secretion may also contribute to an increase in intraocular pressure.
In addition, ocular inflammation is typically treated with corticosteroids, and in steroid-responders this may be an additional factor contributing to increased intraocular pressure. The risk factors identified for a steroid-induced increase in IOP include rheumatoid arthritis, diabetes, younger age and a family history of glaucoma.
Secondary angle closure may occur due to the formation of peripheral anterior synechiae, posterior synechiae (an adhesion between the iris and lens) creating a pupil block, angle neovascularisation and (rarely) obstruction of the angle by the ciliary body, secondary to inflammation.
There are a wide range of possible aetiologies for anterior uveitis, and a detailed discussion of these is outside the scope of this reference, however they can be broadly divided into infectious and non-infections aetiologies (including HLA-B27 associated conditions, juvenile idiopathic arthritis, sarcoidosis, systemic lupus erythematous, Fuch's heterochromic iridocyclitis and Vogt-Koyanagi-Harada disease).
Clinical Signs
Acute anterior uveitis presents with symptoms such as blur, ocular pain, photophobia, haloes around lights and/or a frontal brow ache. On slit lamp examination, cells and flare may be seen in the anterior chamber. These are best visualised with a small beam (1mm by 1mm), with the beam angled at approximately 45 degrees.
Keratic precipitates (KP) may be noted on the corneal endothelium with the type and presentation of these dependent on the cause of the uveitis. In severe cases, there may be an accumulation of white blood cells in the anterior chamber (hypopyon).
Whilst there are several causes of increased IOP in anterior uveitis, a decrease in intraocular pressure may also be noted due to inflammation of the ciliary body.
Case Examples
-
Case 1: Anterior uveitis
A 56 year old symptomatic male presented for a glaucoma assessment. His best corrected visual acuity in the right eye is 6/12- (20/40-) and in the left 6/6 (20/20). His intraocular pressures were 20mmHg (OD) and 19mmHg (OS) in the context of average corneal thicknesses (pachymetry 527µm OD, 519µm OS). A right ptosis was noted.
Slit-lamp examination showed anterior chamber cells and keratic precipitates. Gonioscopy shows angles open to the ciliary body band in all quadrants with no signs of neovascularisation or synechiae.
He was referred to an ophthalmologist for further assessment and management of the anterior uveitis.
Anterior eye photograph (right eye)
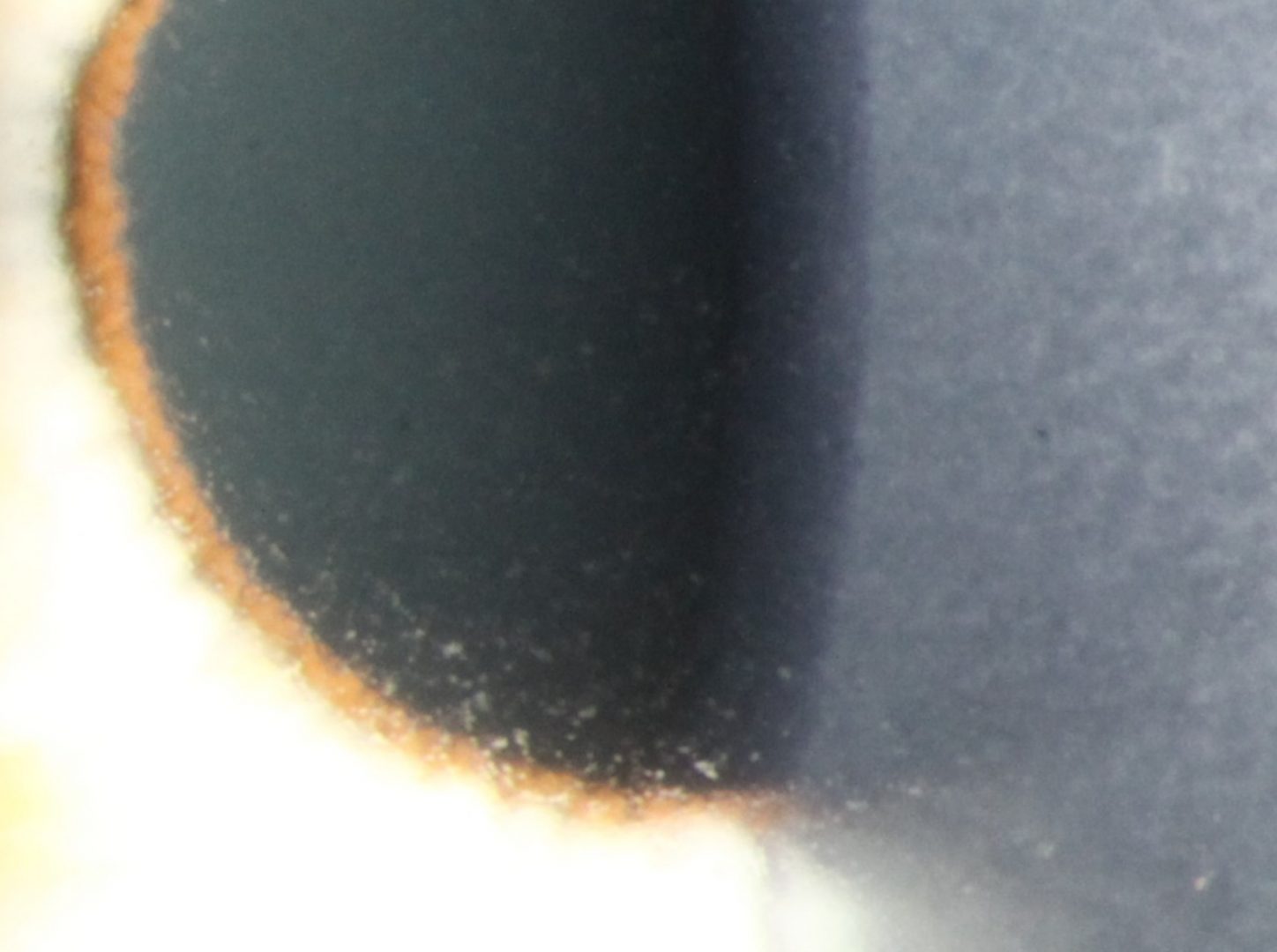
More infoMagnified image of a beam showing cells in the anterior chamber (right eye)
More infoFundus photographs (right and left eye)
More infoRed-free images (right and left eye)
More infoMagnified image of the right and left optic discs
More infoCirrus RNFL Analysis
More infoCirrus Ganglion Cell Analysis
More info24-2 SITA-standard visual field analysis
More info -
Case 2: Fuchs' heterochromic iridocyclitis
A 67 year old male with a history of recurrent anterior uveitis and increased intraocular pressure following use of topical corticosteroid treatment. The last episode of uveitis was 4 months previous, however he has noticed symptoms in his left eye developing over the last 1-2 days. Visual acuity is 6/6 in each eye. Intraocular pressures are 12mmHg (OD) and 29mmHg (OS), as compared with the patient's previous examination where these pressures were 14mmHg (OD) and 17mmHg (OS). These measurements are in the context of average corneal thicknesses (571µm OD, 579µm OS).
Gonioscopy showed the angles to be open to the ciliary body band in all quadrants.
Features that are consistent with Fuchs uveitis, which in contrast to other types of anterior uveitis, presents with mild symptoms, mild anterior chamber reaction and disproportionately high intraocular pressures. It may also present with iris heterochromia and stellate keratic precipitates. It is a chronic uveitis that is not responsive to corticosteroids and management focuses on treating IOP elevation. Given the elevated IOPs in the left eye, this patient requires initiation of IOP-lowering therapy.
Anterior eye photograph (left eye)
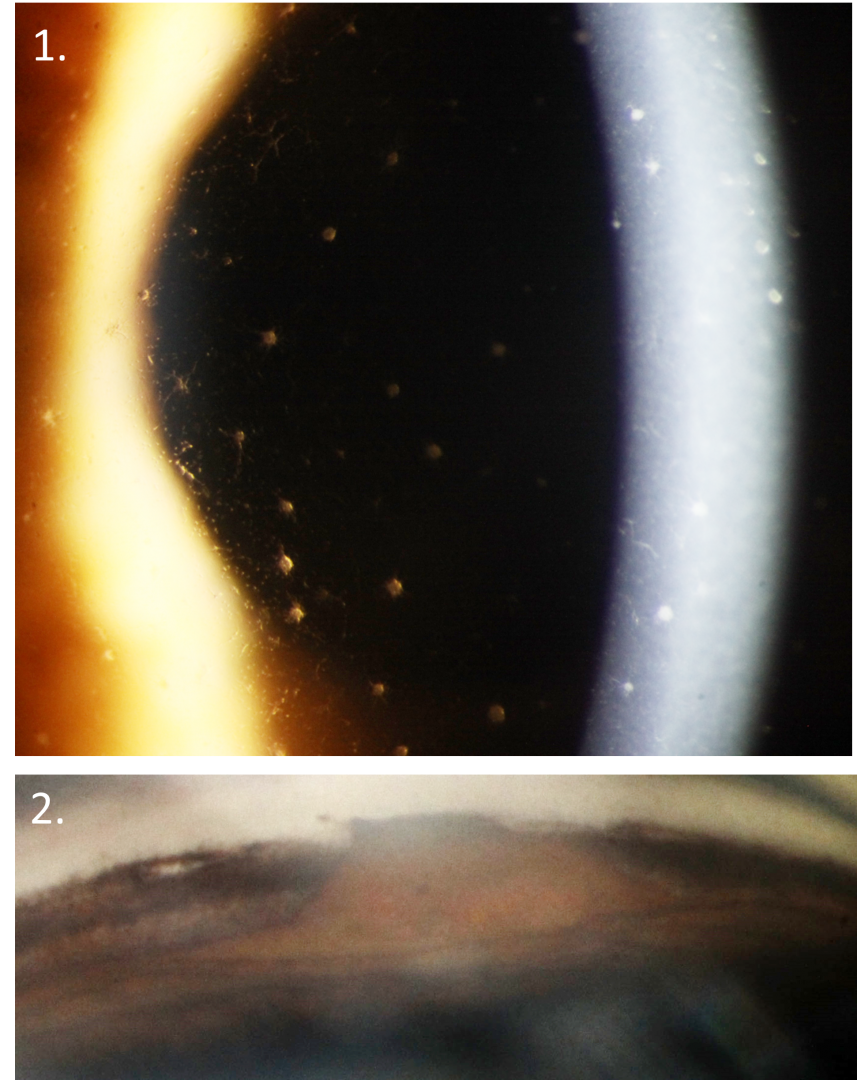
More infoRetroillumination used to show iris transillumination defects (left eye)
More infoFundus photograph and red-free image (left eye)
More infoStereophoto (left optic disc)
More infoCirrus RNFL Analysis
More infoCirrus Ganglion Cell Analysis
More info24-2 SITA-Faster visual field analysis
More info
Differential Diagnosis
References
Bodh SA, Kumar V, Raina UK, Ghosh B, Thakar M. Inflammatory glaucoma. Oman J Ophthalmol. 2011;4(1):3-9.
Jabs DA, Nussenblatt RB, Rosenbaum JT (2005). Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005 Sep;140(3):509-16. 3.
Muñoz-Negrete FJ, Moreno-Montañés J, Hernández-Martínez P, Rebolleda G. (2015) Current Approach in the Diagnosis and Management of Uveitic Glaucoma. Biomed Res Int. 742792.