
Overview
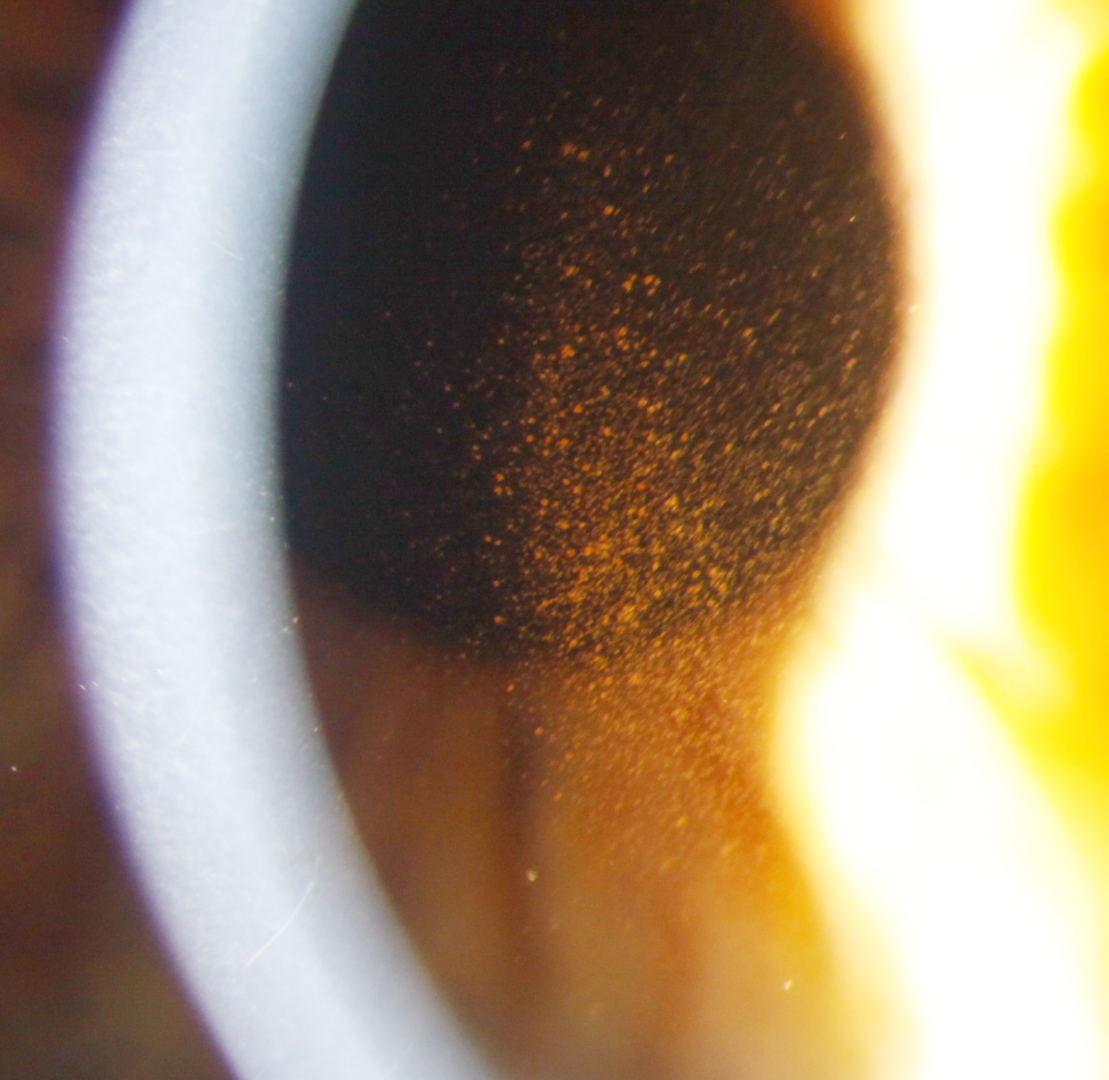
Pigment dispersion syndrome is typically associated with an anomalous iris profile (posterior bowing), causing increased contact between the lens zonules and iris. It is thought that this contact results in a mechanical liberation of pigment from the iris, leading to the characteristic midperipheral, radial iris transillumination defects. Once liberated, the convection currents within the aqueous cause this pigment to be deposited vertically on the corneal endothelium and in the anterior chamber angle.
Deposition of pigment in the trabecular meshwork may impede aqueous outflow and lead to an increase in IOP. The lifetime risk of conversion from pigment dispersion syndrome to pigment dispersion glaucoma has been estimated to between 35 and 50% (Ritch et al. 2000). The risk of pigment dispersion glaucoma is not related to the amount of pigment deposition in the trabecular meshwork, however the severity of pigment dispersion glaucoma is related to the degree of pigmentation (Niyadurupola et al. 2008).
With age, morphological changes in the crystalline lens can reduce the concavity of the iris and cause the zonules to move away from the iris. At this stage, PDS enters the "burnout" phase where pigment release decreases. This burnt out phase is chararacterised by filling in of the iris transillumination defects, reduction of pigmentation on the corneal endothelium and anterior chamber angle and lowering of IOP. On gonioscopy, the 'pigment reversal sign' can be noted where the pigmentation of the trabecular meshwork is heavier in the superior quadrant compared to the inferior quadrant.
Clinical Signs
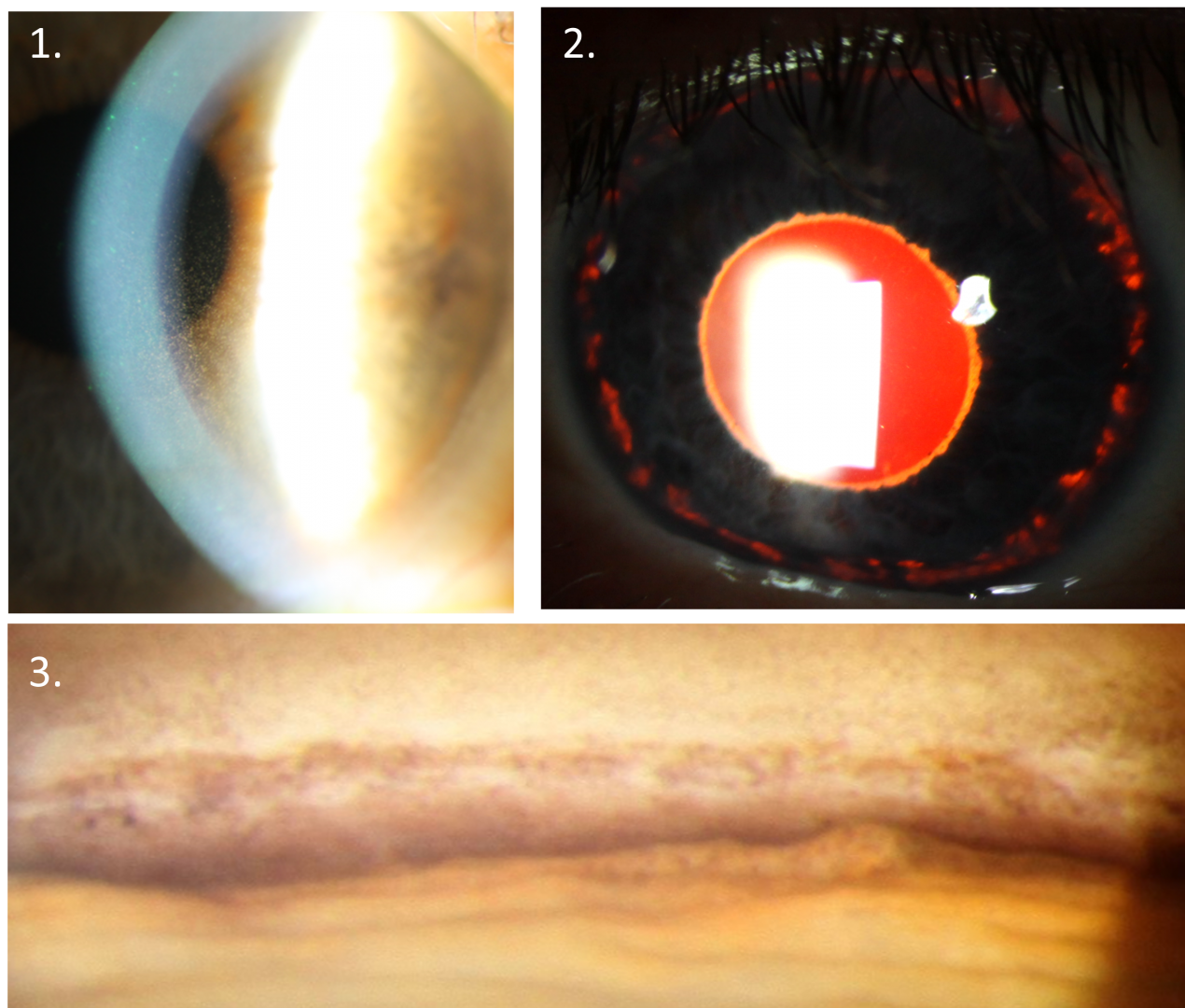
Pigment dispersion syndrome is typically characterised by the presence of 3 key clinical signs - pigmented cells deposited vertically on the corneal endothelium (1-Krukenberg's spindle), mid-peripheral iris transillumination defects (2) and increased, uniform pigmentation of the trabecular meshwork on gonioscopy (3). The pigment deposited in the trabecular meshwork is typically uniform in distribution, in contrast to the patchy pigment deposition seen in pseudoexfoliation syndrome.
Strenuous exercise may cause pigment liberation, leading to a spike in intraocular pressure. This may in turn give rise to symptoms such as headaches and blurry vision.
Case Examples
-
Case 1: Active pigment dispersion syndrome
A 30 year old male with intraocular pressures of 27mmHg in each eye in the context of thick corneas (central corneal thickness 590µm OD, 605 OS).
-
Case 2: Burnt out pigment dispersion syndrome
A 52 year old Caucasian male with intraocular pressures of 16mmHg in each eye, in the context of average corneal thicknesses (531µm OD, 532µm OS).
-
Case 3: Pigment dispersion glaucoma
A 56 year old Caucasian male with intraocular pressures of 19mmHg in each eye in the context of average corneal thicknesses (567µm OD, 561µm OS).
Gonioscopy of the inferior (1) and superior (2) angles
More infoFundus photography (right and left eye)
More infoRed free images (right and left eye)
More infoOptic disc photos (right and left eye)
More infoCirrus RNFL analysis
More infoCirrus Ganglion Cell Analysis
More info24-2 SITA-Standard visual field analysis
More info
Differential Diagnosis
References
Niyadurupola, N. Broadway DC (2008). Pigment dispersion syndrome and pigmentary glaucoma - a major review. Clinical and Experimental Optometry 36:8868-882.
Okafor, K. , Vinod, K. & Gedde, S. (2017). Update on pigment dispersion syndrome and pigmentary glaucoma. Current Opinion in Ophthalmology, 28 (2), 154-160.
Ritch R. Mudumbai R. Liebmann JM. (2000) Combined exfoliation and pigment dispersion: paradigm of an overlap syndrome. Ophthalmology 2000; 107:1004–1008.