
Overview
The current classification scheme for AMD uses the scheme by the Beckman Initiative for Macular Research Classification Committee. This grading scheme is based on findings within two disc diameters of the fovea in patients older than 55 years of age. The paper by Ferris et al. (Ophthalmology, 2013) outlines this classification and the tabs below link to some case examples of each classification.
This classification scheme is designed to estimate the five year risk of progression to late AMD based on the clinical findings of drusen and pigmentary abnormalities (see below).
To better understand the discussion on this page, it is advisable to have a good understanding of both how we estimate drusen size and the clinical appearance of both drusen and pigmentary abnormalities. Each of these sections can be reviewed by clicking on the appropriate link at the bottom of the page.
Classification
Normal Ageing Changes
Drupelets (diameter less than 63µm) at the macula with no pigmentary abnormalities.
Early AMD
Small to medium sized drusen (63-125µm) at the macula with no pigmentary abnormalities.
Intermediate AMD
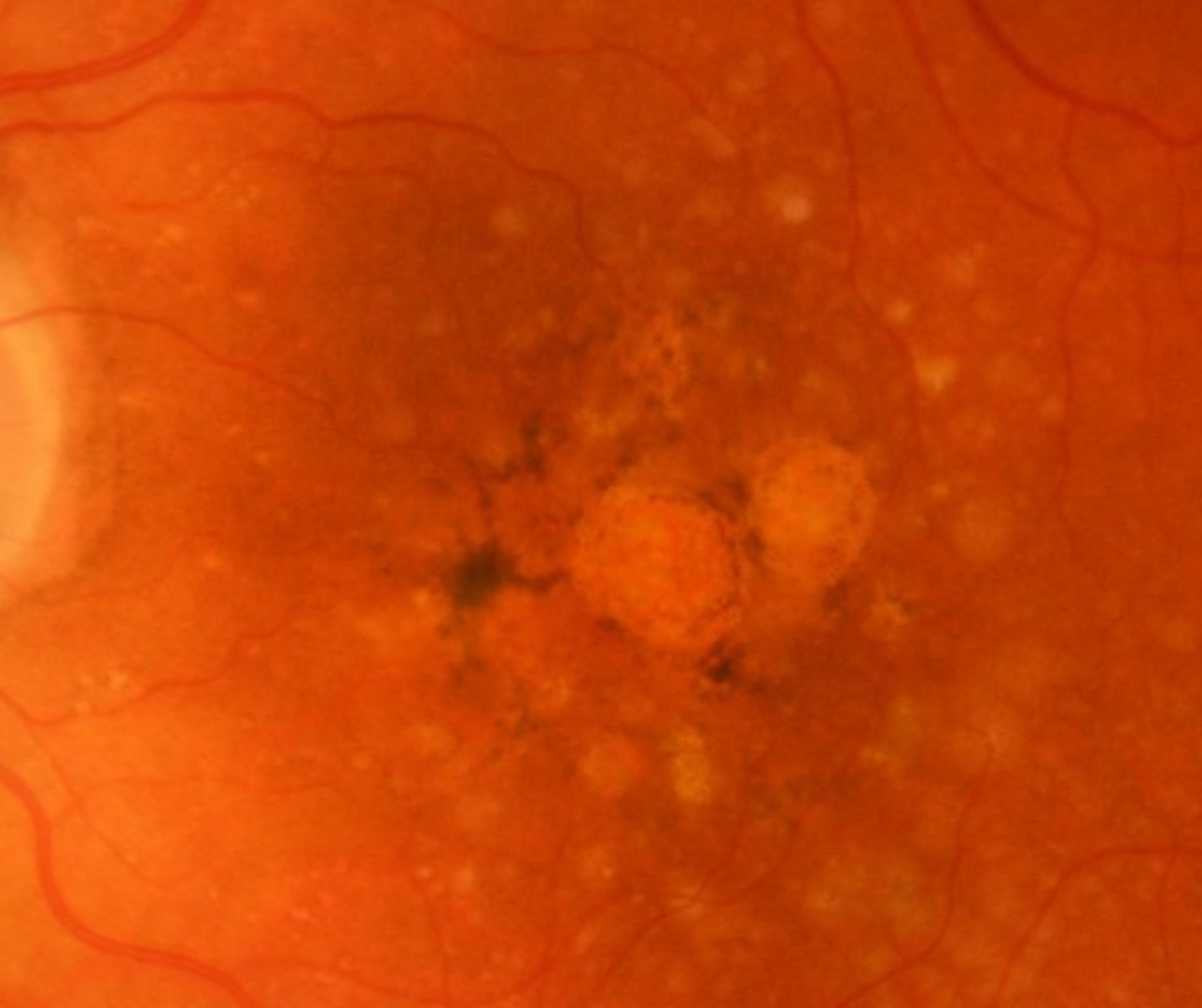
Large drusen (greater than 125µm in diameter) and/ or any pigmentary abnormalities (hyper- or hypo-pigmentary changes associated with at least medium drusen).
Late AMD (Geographic atrophy)
Presence of well demarcated areas of complete atrophy of the outer retina, RPE and choriocapillaris of at least 250 µm in diameter.
Late (Neovascular) AMD)
Presence of macular neovascularisation (MNV) or disciform scar from previous MNV.
Estimating Progression Risk
The AREDS Simplified Severity Scale is a risk factor scoring system for patients with AMD to estimate the risk of progression to late AMD within five years. Developed over 2 decades ago, this scale has been a useful clinical tool for some time.
To calculate risk, apply one risk factor for each eye that has large drusen present, one for each eye that has pigmentary abnormalities at the macula. If neither eye has large drusen, one point is still assigned if there are medium-sized drusen in both eyes. Based on the number risk factors, the risk of progression from intermediate to late AMD within 5 years can be estimated. The original scale estimated this at 0.3% (1 risk factor), 12% (2 risk factors), 25% (3 risk factors) and 50% (4 risk factors).
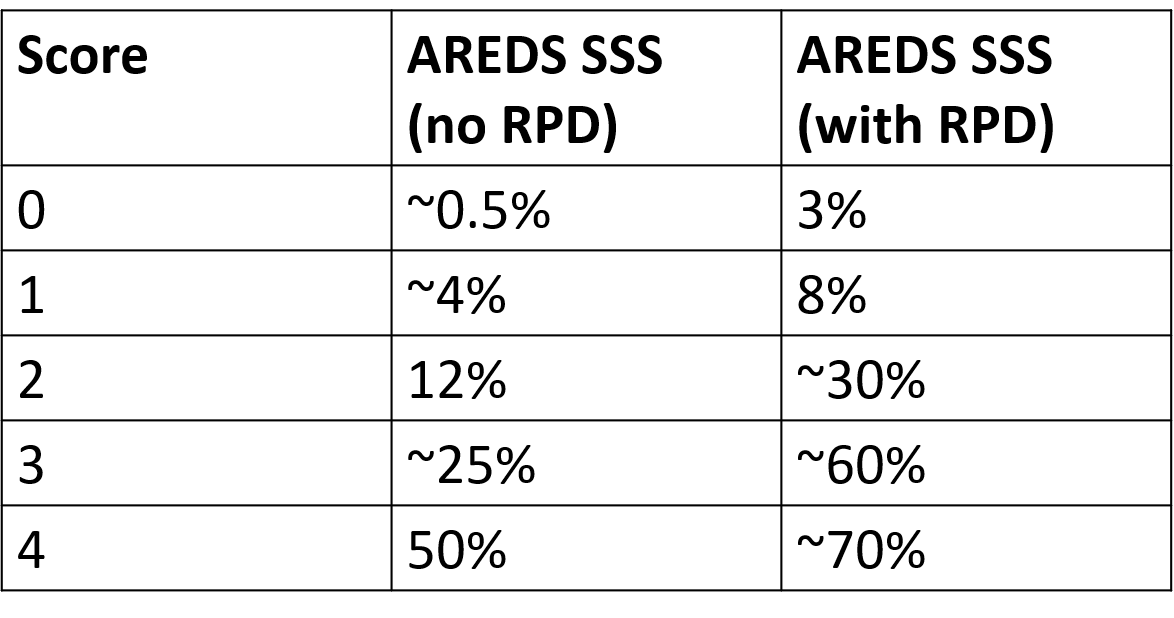
In 2024, results of a post-hoc analysis conducted on 2 trial cohorts (AREDS and AREDS2) were published that stratified this risk according to the presence or absence of reticular pseudodrusen (RPD). A clinical description of RPD may be found on the link below "Intermediate AMD: Prognostic Biomarkers".
Risk of progression in the presence and absence of RPD is shown in the table opposite.
While there is still debate on the validity and utility of predictive biomarkers such as RPD, the evidence at present suggests that clinicians should proactively incorporate the detection of RPD into their examination of AMD patients, and consider the presence of RPD when determining appropriate review periods.